Dave Asprey — How Ketones May Be Useful Against COVID-19
This article was previously published June 7, 2020, and has been updated with new information.
In this interview, Dave Asprey, a Silicon Valley entrepreneur, founder and CEO of bulletproof.com, and author of "The Bulletproof Diet" and "Head Strong: The Bulletproof Plan to Activate Untapped Brain Energy to Work Smarter and Think Faster — in Just Two Weeks," discusses the role ketones play in COVID-19.

The initial motivation for this interview was the recent passing of Richard Veech, M.D., Ph.D., a Harvard trained physician who then went to Oxford to train with biochemist Sir Hans Krebs. Veech was a pioneer of the ketogenic diet and believed ketones have powerful antioxidant effects. This aligns with Asprey’s experience as well. As noted by Asprey:
"Your mitochondria's job is to take air and food and convert them into energy. If it does a complete job of that, you stay lean, you don't get inflammation and you have lots of energy.
[In] that complex process that Veech worked with Hans Krebs on — the Krebs cycle — parts of it are broken, you end up getting electrons that don't go where they're supposed to, and you end up with inflammation … these inflammatory cytokines throughout the body."
How to Raise Your Ketones
Veech developed and was fond of ketone esters, but they tend to be expensive. Two brands that make ketone esters are HVMN and KetoneAid. The alternative, beta-hydroxybutyrate salts can, according to Veech, cause mitochondrial harm, which is why he didn't recommend them. You can also raise your ketones naturally by going on a very low-carb, high-fat, moderate protein diet. Asprey mentions some additional strategies:
"The way that I pioneered and still prefer, is using certain types of MCT oil. The C8 MCT also will turn into beta-hydroxybutyrate … I do about a tablespoon or two spread out throughout the day …
If you have enough of any of these three forms of ketone-generating things in the body, what happens is those ketones come in, and then the cell says, 'Oh, wait, I could use a unit of oxygen and a unit of glucose or a unit of ketone.' When it uses the ketone, it gets more electricity out of it than it would from the sugar.
Your neurons love this. Your heart cells love this and it tends to wake you up. It tends to make you feel good. And if you've heard of bulletproof coffee, which I'm very well known for … it works because when you put that C8 MCT, the Brain Octane oil, in [the coffee], it gives you ketones so that when your brain is in the state of working, it works.
From the perspective of COVID-19, anything that raises your ketone levels is probably going to be good for you. One of the magic things that raises ketones is eight hours of fasting — that's called sleeping. Plus, the amount of caffeine [found] in two small cups of coffee is shown to double ketone production.
So, what I'd propose is, if you're feeling crappy, and you have COVID-19, you probably should have some coffee. And you probably should have whatever ketones you can possibly get from any of those forms, because it's anti-inflammatory, because it can help your cells with energy.
When you do that, it will likely turn down this inflammatory snowball effect that happens. Even … sepsis … can be prevented by restoring ATP levels, NAD levels and something called the acetyl coenzyme A. So, what we're trying to do is get in before the damage happens."
While Asprey takes 1 to 2 tablespoons of C8 MCT oil a day, I regularly take 12 to 14 tablespoons a day. At 100 calories per tablespoon, it's my primary source of calories. You will need to work your way up, though, as some will experience digestive upset when first starting. At 14 tablespoons a day, I can get my ketone levels to about 6 if I take additional ketone esters, which is difficult to reach even after a week of water fasting.
Insulin Resistance Makes You Susceptible to Cytokine Storm
According to recent NHANES data,1 87.8% of Americans are metabolically inflexible and, as such, are at an increased risk of developing COVID-19 due to impaired immune function. Diabetes, high blood pressure, obesity and elevated fasting triglycerides are all clinical symptoms of insulin resistance.
When you burn sugar for fuel, you need to break glucose down to two molecules of 3 carbon pyruvate. Pyruvate is then used by your mitochondria after it is converted to acetyl CoA. Insulin resistance, in turn, can impair the enzyme that converts a breakdown product of glucose into pyruvate so it can be shuttled and burned as energy in your mitochondria.
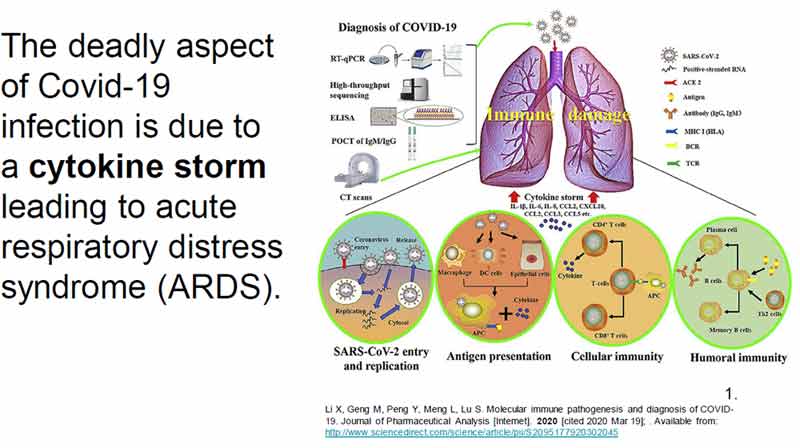
Ketones Inhibit Cytokine Storm
The problem with COVID-19 is that the cytokine storm inhibits the enzyme converting pyruvate to acetyl CoA, which radically limits your mitochondrial ATP production. An additional consequence of this is that it also reduces NADPH.
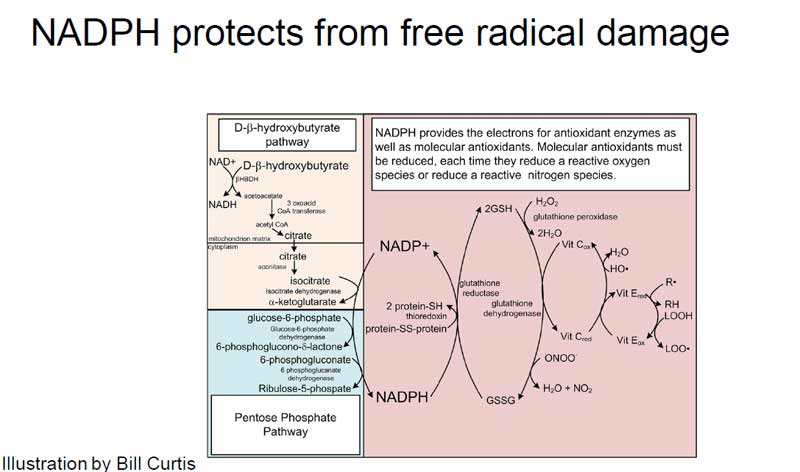
NADPH is the battery of your cell, the reservoir of electrons that actually cause endogenous antioxidants like glutathione, vitamin E and C to be recharged so they can continue to work and mitigate against the free radical damage resulting from all this oxidative stress. One way to compensate is to make sure you have enough NADPH, and ketones radically upregulate NADPH.
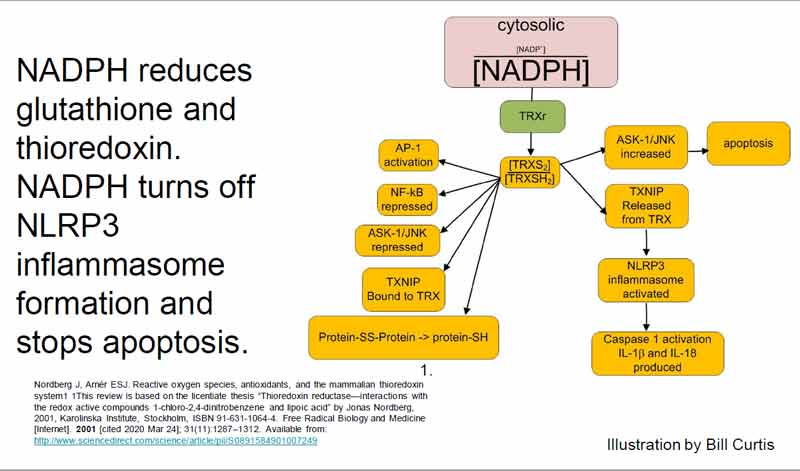
NADPH also turns off NLRP3 inflammasome that produces cytokines like TNF alpha, NF Kappa B, IL1B, IL6 and IL18 (interleukins) that are causing all the damage.
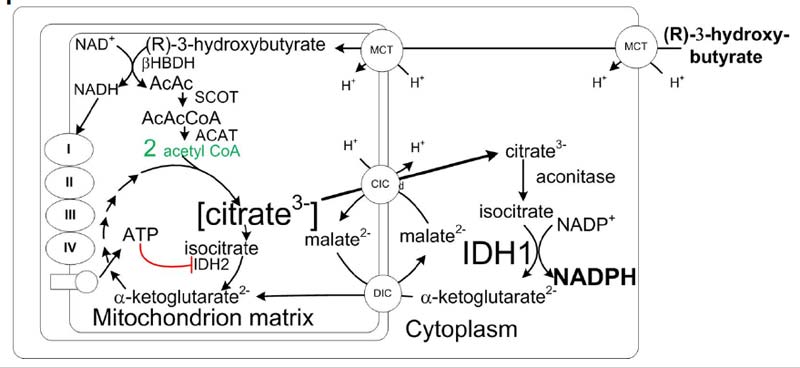
Ketones are also able to interrupt the feedback cascade of cytokine storms caused by ionizing radiation. It is thought that it does this by providing a source of NADPH that is not dependent on glucose or sensitive to pyruvate dehydrogenase kinase or loss of pyruvate dehydrogenase phosphatase. Ketones are also useful for ARDS, stroke, traumatic brain injuries, and radiation exposures such as flying, CT scans, X-rays and 3D cone beam CT scans.
While many of my readers are not metabolically inflexible and therefore at low risk for COVID-19, most are at some point exposed to ionizing radiation exposure. We discuss this at greater depth in the interview, so for more details, listen to it in its entirety, or read through the transcript.
As noted by Asprey, the pathways involved in nutritional ketosis are relatively well-understood, and they point to ketones being a valuable prophylactic and adjunct to COVID-19 treatment.
"I have a little pulse oximeter on my finger right now. It's a $30 item, and it tells you what your blood oxygen level is. [Mine's] at 98%. It will probably go to 99% in a minute. What's going on here is my lungs are working fine and my blood can carry oxygen.
When people get COVID-19, and they're not metabolically healthy, then [their oxygen level] could be at 90 and [they] feel a little bit weird. But they're actually metabolically really broken and their blood is starting to break down from [SARS-CoV-2 infection] and they're starting to get the inflammatory cytokine storm.
If they had ketones present, if they were able to measure [their oxygen level], if they could block a cytokine storm with any of the herbs that we know about — andrographis stands out really well, but so does oregano, bay leaf, rosemary, green tea — if they could block iron using vitamin C, they wouldn't be getting the lung damage and they might not even have to go to the hospital.
I just wish that the knowledge was out there, but when we have authorities saying, 'Well, there's nothing approved or studied for this,' what that means is 'don't do anything until we say so,' which is a terrible idea."
COVID-19 Patient Successfully Using Ketone Esters
Below, I've included a video of a COVID-19 patient who, when given ketone esters, experienced significant improvement in her breathing — within minutes.
While the ketone esters provide fairly astounding improvements in COVID-19, they are in no way treating the primary cause of the disease, which is an impaired immune system, typically due to insulin resistance. This is why it is key not to rely on ketone esters as a magic bullet but, rather, a powerful tool that can be used when needed.
The Importance of Magnesium
Aside from ketones, magnesium is also important. "You can't make enough of the chemicals that you need to make to fight off an inflammatory cytokine storm if you don't have high magnesium levels," Asprey notes. "And you won't be able to have enough ATP because you get calcium dysregulation if you don't have enough magnesium."
Asprey recommends taking 500 milligrams to 1,500 mg of magnesium each day if you're taking ketone esters, ketone salts or MCT oil. Like me, Asprey prefers magnesium threonate, as it has better absorption into the brain and doesn't cause loose stools even at high doses. But he also takes other forms of magnesium.
"I take mixed magnesium-ate. In other words, every form of magnesium that ends in 'ate' [such as] orotate, citrate, malate. So, I'm getting broad spectrum in the evening and the brain one [magnesium threonate] in the morning."
Aside from magnesium threonate, one of my favorite forms of magnesium is molecular hydrogen tablets. Once dissolved in water, each tablet liberates 80 mg of highly absorbable ionic elemental magnesium. On a side note, Tyler Lebaron, founder of the Molecular Hydrogen Institute, did a magnificent lecture on the therapeutic value of molecular hydrogen for COVID-19 and the molecular biology behind it, so it can be beneficial in more ways than one.
Metabolic Inflexibility Is the Primary Risk Factor
The primary risk factor for serious COVID-19 infection is metabolic inflexibility. Crazy enough, research2 published in Metabolic Syndrome and Related Disorders in February 2019 concluded that 87.8% of the U.S. adults sampled were metabolically inflexible.
A mere 12.2% met the updated guidelines for metabolic health. Among the overweight, only 8% were metabolically healthy and among the obese, only 0.5% met the criteria for metabolic health. As noted by the authors:3
"Prevalence of metabolic health in American adults is alarmingly low, even in normal weight individuals. The large number of people not achieving optimal levels of risk factors, even in low-risk groups, has serious implications for public health."
We're certainly seeing the implications for public health in this pandemic. One of the most effective ways to regain your insulin sensitivity and metabolic flexibility is through time-restricted eating. The ability to burn fat and generate ketones is how you know that you're metabolically flexible. Alternatively, you could do cyclical fasting.
"When I was obese, I knew I would starve if I didn't eat six times a day, which is totally wrong. Now, I have two kids. They're 10 and 12. That week, they both said, along with my wife, Dr. Lana, 'We're going to fast for 24 hours.' So, we had dinner and we didn't eat anything until the next day's dinner.
And you know what, the kids handled it … They played and did their farm chores and it wasn't a big deal. I like to think, 'Great, I have metabolically flexible kids.' If you're not doing this kind of a practice, then OK — anything that quickly stresses the cells and then allows them to recover will help metabolic flexibility.
So, you could try cold showers … Getting quality sleep is another way … And if you're going to exercise, do very brief, very intense exercise … I'm talking 20 seconds of the craziest thing you can do twice in seven minutes.
Nothing else will outperform a 45-minute steady state cardio workout, according to research from the University of Colorado. All of those things help, but if you have some ketones present when you're doing them, I think you're going to benefit more from all of those."
Other Mechanisms of Ketones
Ketones are also a histone deacetylase (HDAC) inhibitor, which has profound metabolic implications. By inhibiting HDAC, ketones radically reduce inflammatory consequences like cytokine storms. Ketones also activate Nrf2 and FOXO3a, transcription pathways that decrease oxidative stress by increasing endogenous antioxidants.
So, overall, ketones push everything in the right direction — away from inflammation. It's much more difficult to get into trouble with inflammation when your ketone level is high. Asprey agrees, saying:
"It's true. Now we've got millions of people who are stuck at home, and a lot of them are saying, 'Oh, I can't afford this stuff, it's too much.' But at the end of the day, you are so much less hungry. And we're talking about skipping meals.
It is cost-effective to put 100 calories of MCTs into your diet every day, even if you're on a pretty restricted diet, because it does so much good stuff for you. And it replaces some other oils that you're going to pay for and it makes you not hungry.
So, I am advising people, the more soluble fiber and the more MCTs you can take right now, the better off you're going to be. And then, of course, avoid the industrial meats and the fried stuff and the bad oils. If you can do that … [COVID-19] illness will be very different than if you don't do that. And, of course, you have to exercise and all that."
Hyperbaric Oxygen
Another amazing tool discussed in this interview is hyperbaric oxygen. It’s a particularly valuable alternative to mechanical ventilation.
Mechanical ventilation can easily damage the lungs for the fact that it's pushing air into the lungs with force in a disease where the alveoli are compromised and filled with fluid from inflammatory cytokines due to insulin resistance. HBOT bypasses this problem by supplying 100% oxygen in a pressurized chamber, which allows your body to bypass this defect and absorb oxygen directly into your tissues.
Opelousas General Hospital in Louisiana, which has a hyperbaric center, has been deploying "off-label compassionate use" of HBOT as an alternative for patients that would otherwise have required ventilation.4 So far, 100% of patients treated with HBOT saw rapid improvements in their respiratory rates and dramatic decreases in CRP (an inflammatory marker) and D-dimer (a measure of blood coagulation), and none has required ventilation.
Reducing Comorbidity Factors Is Essential Pandemic Response
However, as important as it is to have effective treatments, it's even more important to address the underlying causes to prevent out-of-control infection in the first place.
"The whole idea of flattening the curve is such a cowardly, low-end goal," Asprey says. "The goal ought to be to lower the curve, because those of us who do math understand that if you flatten the curve, it's the same number of people who get sick [in the end]. You got sick later so we could have more doctors for you.
What I want is fewer people to get sick. [By reducing comorbidity factors] we'd take the load off the medical system, which is an important goal, but we'd also [reduce] the chance of dying, we'd lower the overall death rate, and you do that through prevention. That's been entirely missing from the $2 trillion national strategy, which is astounding to me.
When you look at what's really going on inside the body, there is systemic hypoxia. We have three different studies that show that hemoglobin is pulled apart and iron comes out, using three different methodologies, which is very fascinating. And then there's all the field reports of people saying, 'Why are my patients hypoxic, yet their lungs are still working?' …
Let's see. Heart damage, brain damage, neurological symptoms, loss of smell and taste. Any high-altitude mountaineer like me will tell you, you can't taste your food at high altitude. There's a reason for that. And they're also seeing those red spots on their feet, which are furthest from the heart and get the lowest amount of oxygen.
So, every symptom that has been documented from COVID-19 is hypoxic-related except for damage to the lungs, which is iron-related from all the free iron from … the damage to the hemoglobin. So, what do we end up with when you put all that stuff together?
You have a person who is hypoxic. And no matter what you do to their lungs, it doesn't matter because their blood doesn't carry oxygen well. So, how would you address that? Stick them in a hyperbaric chamber … Hyperbaric forces oxygen into the cells without hemoglobin being required.
When you do that, the cells that are struggling [get oxygenated] as the bone marrow works to make more red blood cells. By the way, we have data that COVID-19 makes bone marrow produce more blood cells. We know there are biological markers of that …
Given that these chambers … have other uses for things like traumatic brain injuries, metabolic problems and cancer, this ought to be something every hospital has. [Many] do have [hyperbaric chambers] yet it's usually illegal to use [HBOT for many of these conditions] …"
We Need a Return to Common Sense
As for the direction we're getting from our government leadership and mainstream media, Asprey is like me — frustrated with the lack of common sense and balance.
"You'll see these talking heads on TV saying, 'Well, I have a medical degree and I've spent 40 years studying how to use drugs to treat diseases, and there are no drugs that we have yet proven to treat this disease, therefore, you will sit there and eat pizza.'
I'm like, 'What is wrong with you?' There's this whole body of knowledge and you don't have to do everything I've talked about. You don't have to be able to spell HDAC inhibitor. What we can tell you is, use some MCT oil, get enough sleep, don't eat after dark, intermittently fast and maybe you'll just be harder to kill from any bad disease, and that's OK …
I'm particularly shocked that they're shutting down parks and [beaches]. It doesn't make any sense … The people who won't socially isolate won't socially isolate, but preventing children from having access to sunshine [and] walking in grass — it's mean, it's unnecessary and it's beyond the scope of what our government is legally allowed to do in the U.S.
So, we sometimes need to just say, 'All right, let's do what Sweden's head doctor did.' The people said, 'What should we do? We need guidance.' And he said, 'You're smart people. Use common sense.' And that was literally the guidance …
There are some heinous statements being made at the highest levels saying, 'Science says there's no evidence.' But there is evidence. There's lots of evidence. The fact that one of the seven forms of evidence is double-blinded clinical trials does not mean that [you ignore] when a large number of clinical people treating people notice that something works.
That is a great form of evidence. Another form of evidence is we understand these pathways and A leads to B, leads to C, therefore, C is likely. That is a form of evidence. It doesn't mean it's proof, but it's evidence.
For our leaders to say, 'Hold still, die and lose your businesses and your livelihood while we wait for our preferred form of evidence,' is fear-based decision making. It's dysfunctional … Doing nothing until we know everything, that doesn't work."
If there is a silver lining to this pandemic, it’s that it’s showcasing that healthy lifestyles provide essential immunity to these types of infections and disastrous health consequences. Hopefully, people will start to wake up and recognize there is something you can do that doesn't involve taking medications or vaccines — something that can strengthen your own innate immune system.
To learn more about Asprey's work, be sure to check out his blog, DaveAsprey.com, and listen to his Webby Award-winning podcast, Bulletproof Radio.
from Articles https://ift.tt/3FV1i7g
via IFTTT