Several processes in the roundworm C. elegans boost the stress response in cells, incidentally making worms resistant to a high-fat diet and extending their lifespan. Researchers have found another: cells called glia that release a hormone that boosts the unfolded protein response in the endoplasmic reticulum of the worm's cells, effectively doubling lifespan. This could lead to interventions to tune up peripheral cells, such as muscle cells, and prevent age-related deterioration in humans.
from Top Health News -- ScienceDaily https://ift.tt/38Oi48F
A team took a novel, interdisciplinary approach to analyzing the behavior of breast tumor cells by employing a statistical modeling technique more commonly used in physics and economics. The team was able to demonstrate how the diversity, or heterogeneity, of cancer cells can be influenced by their chemical environment -- namely, by interactions with a specific protein, which leads to tumor growth.
from Top Health News -- ScienceDaily https://ift.tt/37SsC53
Several processes in the roundworm C. elegans boost the stress response in cells, incidentally making worms resistant to a high-fat diet and extending their lifespan. Researchers have found another: cells called glia that release a hormone that boosts the unfolded protein response in the endoplasmic reticulum of the worm's cells, effectively doubling lifespan. This could lead to interventions to tune up peripheral cells, such as muscle cells, and prevent age-related deterioration in humans.
from Diet and Weight Loss News -- ScienceDaily https://ift.tt/38Oi48F
Few studies have examined how the neighborhood's physical environment relates to cognition in older adults. Researchers categorized 4,716 individuals by apolipoprotein E (APOE) genotype -- a genetic risk factor for Alzheimer's disease (AD) to determine if there are cognitive benefits of living in neighborhoods with greater access to social, walking and retail destinations. Results showed that the positive influence of neighborhood environments on cognition are strongest among those who are at the lowest risk for AD, specifically APOE ?2 carriers.
from Top Health News -- ScienceDaily https://ift.tt/38Sr10s
Scientists find that normal intestinal cells 'de-differentiate' en masse into stem cells that generate the cells needed for a healthy intestinal lining. New study establishes de-differentiation as the predominant mode of stem cell recover in the intestine.
from Top Health News -- ScienceDaily https://ift.tt/2ujqENv
Using a machine-learning algorithm, researchers have identified a powerful new antibiotic compound. In laboratory tests, the drug killed many of the world's most problematic disease-causing bacteria, including some strains that are resistant to all known antibiotics. It also cleared infections in two different mouse models.
from Top Health News -- ScienceDaily https://ift.tt/2V9QDSv
A multi-institution study has attempted to tease out the relative impact of two variables most often linked to life expectancy -- race and education -- by combing through data about 5,114 black and white individuals in four US cities.
from Top Health News -- ScienceDaily https://ift.tt/32eBP6I
New research by neuroscientists uses a unique model -- the intricate mating songs of birds -- to show how the intrinsic properties of neurons are closely tied to the complex processes of learning.
from Top Health News -- ScienceDaily https://ift.tt/2SN1ksN
A recent study of indigenous people in southern Chile challenges Western assumptions about children's emotional capabilities and highlights the value of spending time outdoors to help children regulate their emotions.
from Top Health News -- ScienceDaily https://ift.tt/2SKxLrH
Researchers have developed a tiny 'heater' -- about the size of a pill -- that could allow resource-limited regions around the world to test for infectious diseases without the need for specialized training or costly lab equipment.
from Top Health News -- ScienceDaily https://ift.tt/32jVbHM
Researchers have demonstrated the use of stem-cell-derived 'mini-brains' to detect harmful side effects of a common drug on the developing brain. Mini-brains are miniature human brain models, developed with human cells and barely visible to the human eye, whose cellular mechanisms mimic those of the developing human brain.
from Top Health News -- ScienceDaily https://ift.tt/37Ksdlq
Investigators successfully measure brain temperature in newborn babies undergoing therapeutic cooling, showing that the treatment effectively targets the core of the brain.
from Top Health News -- ScienceDaily https://ift.tt/2VdoRVg
A first cell atlas of the human thymus gland could lead to new immune therapies to treat cancer and autoimmune diseases. Researchers mapped thymus tissue through the human lifespan to understand how it develops and makes vital immune cells called T cells. In the future, this information could help researchers to generate an artificial thymus and engineer improved therapeutic T cells.
from Top Health News -- ScienceDaily https://ift.tt/38PcGSH
Ecofriendly materials, produced under good work conditions -- convincing arguments for most of us. But how do consumers really weigh compliance with such ethical standards? Not as much as they think: Researchers used an example from textile industry to demonstrate that customers unconsciously use a single ethical aspect as an excuse for less moral behavior regarding other aspects. They report about these 'indulgence effects' and their significance in a recent article.
from Top Health News -- ScienceDaily https://ift.tt/3a4svFp
We’ve all been there. You awaken in the morning and one of your hands is completely numb. It feels dead, heavy, and simply won’t work. Perhaps there’s some tingling as well. Or, you arise from a long dinner or movie and one of your legs feels that way. Then over a few minutes — maybe you shook your hands, stamped your foot — everything goes back to normal. Until the next time.
The first time this happened, it might have been worrisome. But, now that you know it’s temporary and happens to everyone, it may not bother you. But did you ever wonder why in the world this happens? Read on!
When the nerves are not happy
When someone complains to me about their hand or leg falling asleep, I reassure them. I usually explain, “The nerves are not happy.” In general, numbness, tingling, and other symptoms called paresthesia are most commonly due to abnormal nerve function. And when this is intermittent, temporary, and related to holding one position for a long time, it’s rarely anything to worry about. The cause in these cases is simply pressure on one or more nerves travelling into the hands or feet. When you remove the pressure (by changing position, for example), the problem goes away.
However, many other causes of nerve problems — more than 100, in fact — can cause similar, though more prolonged and persistent, symptoms, as noted below. If you have one of these conditions, you’re far from alone: an estimated 20 million people have a form of peripheral neuropathy that might make hands or feet numb or tingly.
A word on nerve terminology
So, what is peripheral neuropathy? It’s worth clarifying some commonly used medical terms.
Neuropathy means nerve disease.
Peripheral neuropathy is a condition affecting nerves in the peripheral nervous system, which includes nerves outside of the brain and spinal cord. Nerves of the legs and arms are part of the peripheral nervous system, and tend to be the first ones affected by diseases of peripheral nerves.
Compression (or entrapment) neuropathy develops because of pressure on a nerve. Carpal tunnel syndrome, which occurs when a nerve becomes compressed in an already tight channel in the wrist, is one well-known example. Having your hand or foot fall asleep is another. Fortunately, this is quite temporary, while carpal tunnel syndrome is often chronic.
Paresthesia is a sensation of pins and needles, numbness, or another abnormal sensation, often tied to peripheral neuropathy. Having your hand or foot fall asleep is a temporary paresthesia.
When to see your doctor
If you’re hands or feet fall asleep occasionally and normal sensation quickly returns, that’s fine. No need to contact your doctor.
But call your doctor promptly if you have persistent numbness, tingling, or other unusual sensations in your hands or feet. This is especially important if these sensations cause trouble with walking or holding onto things. Your doctor should investigate further and will likely consider possible causes of peripheral neuropathy, including the following:
Diabetes is the most common identifiable cause of peripheral neuropathy, accounting for nearly a third of cases. Sometimes it’s the first indication that a person has diabetes.
diseases of the liver, kidney, and thyroid
nutritional deficits, such as vitamin B12 deficiency or other vitamin deficiencies. Vitamin B6 is unique in this regard because too little or too much can cause neuropathy; too little is quite rare, but it’s possible to get excess B6 from supplements.
alcohol and other toxins. Alcohol ingestion is probably the most common cause of toxic neuropathy. Alcoholics may also have nutritional deficiencies that can cause neuropathy.
Certain medications, including some antibiotics and chemotherapy drugs, or lead, mercury, and other chemical and industrial toxins, may be culprits.
vascular disease, which occurs when the blood supply to a peripheral nerve is impaired, as with atherosclerosis. The nerve becomes unhealthy or dies.
Additional causes of neuropathy are infection, compression or trauma to nerves, and inflammatory or autoimmune conditions that affect nerves. It’s worth noting that nearly a third of cases have no clear cause — a problem known as idiopathic neuropathy.
The bottom line
The causes of peripheral neuropathy are many, and range from the harmless and annoying to the intolerable and dangerous. When in doubt, see your doctor. But try not to worry when your hands or feet fall asleep due to holding your arms or legs too long in one position, as long as this resolves within minutes and doesn’t happen often. These things happen.
And the next time you see a movie, don’t forget to change positions, stretch, and fidget a bit — even if the movie is really good.
We may mistakenly believe that the chances of dying are greater in the air than on the road because the severity of aviation accidents can be devastating. Compare that to automotive accidents where the probability of dying in a given automotive accident is about one half of 1 percent. Here’s the rub, unfortunately: nearly 18,000 automotive accidents occur every day in the US, on average.
This frequency multiplied by the low severity still amounted to nearly 37,000 automotive fatalities in 2018. To put this difference into perspective, between 2000 and 2018 there were 778 fatalities from US scheduled air travel. Over the same time span, there were 723,530 automotive fatalities — almost 1,000 times greater than the number of fatalities from scheduled air travel.
These numbers should scare anyone. If I die in the next 10 years, the most probable “murder weapon” is my vehicle or another vehicle on the road. Is there anything I can do to lower the chances of dying in a car or from a car? Of course, never stepping foot in a car again would drastically lower my chances, but there are trade-offs in life. Before I get into my risk-reduction strategy, a few statistics are in order to inform it.
Also, a caveat: for this analysis, I’m only interested in the driver and what he or she can do to lower the risk of death. I care a lot about pedestrians and other occupants in the vehicle, but to do this analysis, I must remove them from the equation.
Of all drivers killed in US automotive accidents in 2017, 18% occurred on a freeway. This is actually lower than I expected. I think this speaks to a more controlled environment where an interstate must meet federal standards and includes fully controlled access (i.e., entering and exiting is confined to on and off ramps) and a median width of at least 50 feet.
Perhaps the biggest reason why we don’t see more fatal crashes on freeways is that there are no intersections on them (with a few exceptions). In fact, there are more drivers killed in intersections (20%) than on freeways.
After accounting for freeways (18%) and intersections and junctions (20%), we’re still left with more than 60% of drivers killed in automotive accidents left accounted for.
It turns out that drivers killed on rural roads with 2 lanes (i.e., one lane in each direction divided by a double yellow line) accounts for a staggering 38% of total mortality. This number would actually be higher, except to keep the three categories we have mutually exclusive, we backed out any intersection-related driver deaths on these roads and any killed on 2-lane rural roads that were classified as “freeway.”
So, to recap, 3 of out every 4 deaths in a car occur on the freeway, at an intersection/junction, or on a rural road with a single lane in each direction. Let’s double-click on each one of these categories and see if we can answer two very important questions:
What driving error resulted in the fatality?
Who is most likely to be at fault and what was the underlying cause of the error? (One way to think about this question is through the lens of manslaughter versus accidental suicide — was the driver effectively killed by someone else making a mistake, or by a mistake they made?)
If we can answer these questions, we may gain insight into what we can do to lower our risk of death (and the death of others) while driving.
In the cases where drivers are killed on freeways, 31% of them have alcohol in their system and nearly 85% of these drivers were over the legal limit of 0.08 g/dL. Furthermore, 29% of all driver deaths involved speeding, and just under 1 in 10 involved distracted driving.
It’s difficult to get mutually exclusive and collectively exhaustive data here, and there are often multiple related factors. For example, it’s not uncommon for a driver to die on a freeway while speeding and over the legal limit of alcohol.
The primary conditions that lead to fatalities, then, are: alcohol, speeding, and distraction leading to a loss of control or contact with another vehicle. Who is likely to be at fault on a freeway, the driver that was killed, or another driver on the road? It’s not exactly clear from the data, but that doesn’t change our strategy. Why? I think the steps below make it clear.
Rule #1: Consider the conditions above as your not-to-do list to reduce the risk of accidental suicide: Do not drive with alcohol in your system, even if you are (or think you are) below the legal limit. Do not speed. Do not text and drive. Do not get behind the wheel if you are sleep-deprived.
Rule #2: Assume others are not adhering to Rule #1. In particular, assume one person awoke today with the explicit instruction to kill you with their car. If you knew this, how vigilant would you be? How much more closely would you pay attention to each other driver around you? That person swerving around or braking too late? That person looking at their phone? That person speeding up behind you? Look for the killer. Be vigilant at all times, and make sure today is not his day.
Let’s move to the next category of fatalities — intersections and T-junctions. I learned something from one of my best friends in high school who is a long haul truck driver. Talk about someone having a front-row seat to vehicular manslaughter.
He told me many years ago that when approaching an intersection, with the right of way, he always looks left first, then right, before entering. Why? The data below show you what his intuition suggested and his experience crystalized.
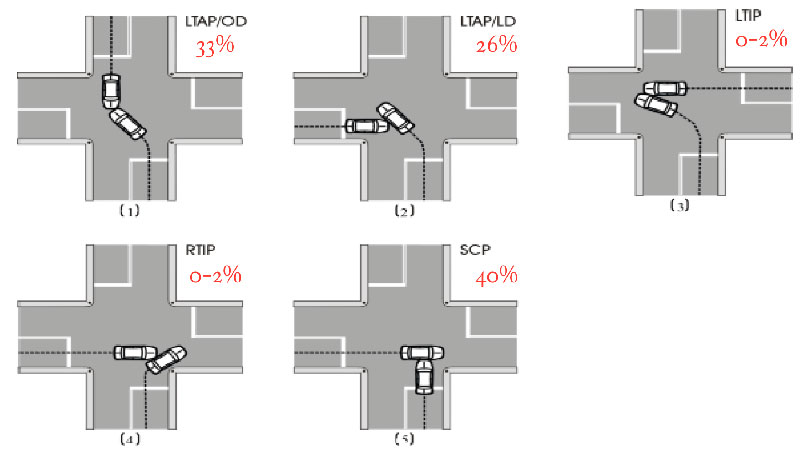
Let’s start with intersections. A driver is most likely going to be struck near the driver’s side by another vehicle, otherwise known as a broadside or T-bone crash. Figure 1 illustrates the different crash scenarios. If a driver is heading through an intersection, with the right of way, the most common cause of his death is the driver on his left, where both cars cross paths, as scenario #2 in Figure 1 most clearly depicts.
Scenario #5, in which two cars go straight through the intersection, has the highest severity. While the figure shows the vehicle heading left to right struck by the one heading up, it’s often the case where the vehicle heading up is struck by the other heading left to right, running a traffic signal or stop sign.
Figure 1. Schematics of, and percent of fatal crashes, Common Crossing Path Crash Scenarios. Fatal crashes include intersections and T-junctions. Figure from the US Department of Transportation.
Legend:
(1) Left Turn Across Path – Opposite Direction Conflict (LTAP/OD)
(2) Left Turn Across Path – Lateral Direction Conflict (LTAP/LD)
(3) Left Turn Into Path – Merge Conflict (LTIP)
(4) Right Turn Into Path – Merge Conflict (RTIP)
(5) Straight Crossing Paths (SCP)
Who is most likely to be at fault when a fatal driver crash occurs at an intersection? It’s often the driver that dies who is the one not at fault. They’re more likely to be obeying the rules of the road, with the right of way, when someone blows a stop sign or traffic light and strikes the victim on the driver’s side, or at an angle.
However, the fault is often shifted to the driver in fatalities occurring at T-junctions. In this case, the driver that’s going to be killed reaches the junction (i.e., traveling up the stem of the “T”) where the road intersects, and proceeds to make a turn before it is safe to do so and is most often struck on the left side by the car traveling in the lateral direction (i.e., heading left-to-right on the horizontal line of the “T”) with the right of way.
This type of accident resembles scenario #2 in Figure 1. The second most common way to get killed is when traveling right-to-left on the “T” and turning left into the stem of the “T” and the vehicle is struck by another heading in the opposite direction. This accident looks like scenario #1 in Figure 1 (you need to rotate the figure 90 degrees left in your mind’s eye for it to match my “T” description for it).
Lastly, let’s turn our attention to the final, and largest, category of deaths. Determining who’s more likely at fault in driver deaths on 2-lane rural roads may be a little bit harder to pinpoint, but we have some clues.
In about 10% of drivers killed in this category, prior to the crash, also referred to as the pre-crash critical event, another vehicle heading in the opposite direction crossed the left lane (i.e., the double yellow line) into the victim’s lane. I think it’s safe to assume that the other driver was responsible for the crash.
However, more often (17% of cases), a driver that is killed on this type of road is the one crossing the lane to his left and encroaching on the opposite lane of travel as the pre-crash critical event. In drivers killed on 2-lane rural roads, 50% involved a driver not wearing a seat belt. Close to 40% have alcohol in their system and nearly 90% of these drivers were over the legal limit of 0.08 g/dL.
About one-third involved speeding, and 16% did not have a valid driver’s license. I think this suggests that driver error plays a larger role rather than another driver at fault. At the least, it suggests that there are some simple things we can do to lower the driver death rate. Which brings me to the larger point of this post.
What are some of the things you can do to improve your chances of not becoming a statistic on the road? The first thing you should do is understand what you should not do.
Speeding is the biggest related factor, involving an estimated 30% of all drivers killed.
Next is being under the influence of alcohol (as well as drugs or medications, the most common being stimulants, that may make drivers more aggressive and reckless, and cannabinols, that may slow coordination, judgment, and reaction times), where 33% have at least some alcohol in their system and nearly 90% of these drivers were over the legal limit of 0.08 g/dL.
After that comes distracted driving (8%), which of course involves the use of mobile phones, failure to keep in the proper lane or running off the road (7%), failure to yield the right of way (7%), and careless driving (6%). I would argue that all of these factors are a form of careless driving (with the exception of some of the crashes involving running off the road).
These are not mutually exclusive factors. I would also argue that the numbers on distracted and drowsy driving (not included above because it’s reportedly involved in only 2% of driver deaths) are underestimated and don’t capture the influence of texting in the case of the former, and the impact of poor sleep in the latter, except in the most extreme cases.
How can you drive more carefully? The best place to start is to look at the factors in the list above and take an honest inventory. As I discussed in the previous email, while there’s no assurance that what I do in a car will keep me alive, I think I can reduce the odds of that happening, beyond simply avoiding these factors, as important as they are.
But, and here’s the key point, assume someone like this person is on the road at all times, and his sole purpose is to kill you. He’s a serial killer and uses his vehicle as his murder weapon. His killing statistics eerily resemble the overall fatal crash statistics. He does a lot of his killings at intersections, but isn’t shy about hopping on the freeway and taking people out there, too.
On the freeways, he may suddenly leave his lane and enter yours within inches of your front bumper, or he’s side by side trying to make contact with your vehicle. Be on the lookout for this maniac.
At intersections, he really likes being on your left and he loves running red lights and stop signs. If you’re going through a green light or a road that intersects with stop signs, look left before you enter and cross the intersection. If you’re at a red light that turns green or proceeding through a stop sign, first look left to make sure the killer isn’t there.
On rural 2-lane roads, he’s been known on occasion to travel in the opposite direction of his victim, leave his lane and force his distracted victims, who traveled these roads so many times they think they can drive them in their sleep, into an avoidance maneuver that results in them driving off the road and rolling their vehicle.
This is where you need to remind yourself that even though you’ve driven these roads countless times without a scratch, it does not give you a pass to be more complacent and lose your focus.
Remind yourself every day to take these measures every time you get behind the wheel. Most of these are obvious and you’ve heard them before, but if you look at the data, my hope is that it makes the steps you can take more tangible.
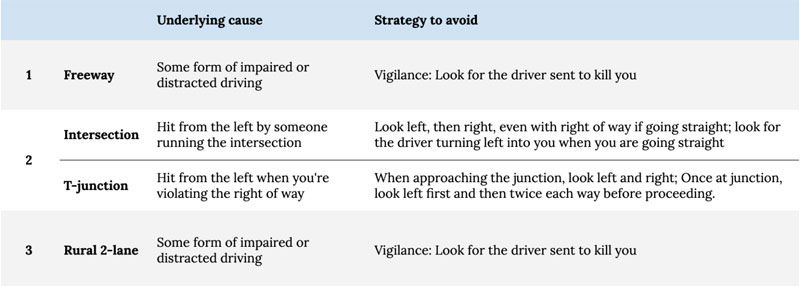
Here in Table 1, I summarize the primary locations of US automotive fatalities, the underlying causes, and most importantly, the steps you can take to reduce your risk of succumbing to them beyond the obvious (Rule #1, above, the so-called not-to-do list).
Table 1. Common causes of driver deaths and additional strategies to reduce their risk.
Before closing this morbid email, one of my patients, who is himself a very frequent helicopter passenger, sent me his rules of engagement for safer flying after reading last week’s email. With his permission, I’m listing them here.
Always fly a twin engine. Two engines are better than one. Statistically, yes, and obvious.
Always “try” to get two pilots. Not because one might have a heart attack (also possible) but to help for visual aid. Watch next time you are in the New York harbor. One pilot is always frantically looking around to avoid the heavy traffic.
If on a crowded helicopter – and they don’t weigh everyone – ask why? It’s actually mandatory on the best-run helicopters.
Always ask for instrument capable pilot and guidance systems.
Always try to avoid bad weather with limited visibility.
About Dr. Attia
Dr. Attia is the founder of Attia Medical, PC, a medical practice with offices in San Diego and New York City, focusing on the applied science of longevity. The practice applies nutritional biochemistry, exercise physiology, sleep physiology, techniques to increase distress tolerance, lipidology, pharmacology, and four-system endocrinology to increase lifespan (delaying the onset of chronic disease), while simultaneously improving healthspan (quality of life).
Millions of people take acetaminophen, commonly known as the brand name drug Tylenol, frequently. People use acetaminophen for treating everything from fevers and muscle aches to headaches, hangovers and other pain. Because acetaminophen is available over the counter and is an ingredient found in many other preparations such as those for cold and flu, few people think twice about taking it. They should.
Acetaminophen is the top cause of acute liver failure in the U.S.1 and overdoses are a leading cause of emergency department visits and hospitalizations.2 According to UT Southwestern Medical Center, more than 200 people a year die from acetaminophen poisoning in the U.S. and there are 15,000 hospital visits due to accidentally taking too much.3
Acetaminophen is also correlated with serious side effects4 such as certain skin conditions, abdominal and gastrointestinal problems and allergic reactions. As I mention later in this article, it also could be dangerous for pregnant women. And, if California state regulators are correct, the latest risk to be associated with acetaminophen may be cancer. The regulators are in the process of determining whether to classify acetaminophen as a carcinogen on the Proposition 65 list.
Public Hearing on Carcinogenicity May Be in Spring 2020
California's Proposition 65, enacted in 1986, requires the state to maintain a list of chemicals known to cause cancer or reproductive toxicity. Businesses are required to provide a warning if the products they sell or use expose the public to chemicals on the Proposition 65 list.5,6
California state regulators reviewed 133 acetaminophen studies in peer-reviewed journals and are considering whether to classify the drug as a carcinogen. They will hold a public hearing in spring 2020. According to The Associated Press, acetaminophen is:7
" … known outside the U.S. as paracetamol and used to treat pain and fevers. It is the basis for more than 600 prescription and over-the-counter medications for adults and children, found in well-known brands like Tylenol, Excedrin, Sudafed, Robitussin and Theraflu. Acetaminophen has been available in the U.S. without a prescription since 1955.
Concerns about its potential link to cancer come from its relationship to another drug: phenacetin. That drug, once a common treatment for headaches and other ailments, was banned by the FDA in 1983 because it caused cancer."
Since the drug is so popular, some fear that a warning will unnecessarily worry the public but Thomas Mack, chairman of the Carcinogen Identification Committee, the group appointed by the governor to identify chemicals linked to cancer,8 dismisses the fears. "That’s not what our mandate is," he says.9
In addition to the tremendous popularity of acetaminophen, inclusion of a chemical on the Proposition 65 list can pave the way for lawsuits, so industry is resisting the classification.10 For example, reports The Associated Press:
"After the state listed glyphosate — widely known as the weed killer Roundup — as a carcinogen in 2017, a jury ordered the company that makes Roundup to pay a California couple with cancer more than $2 billion. A judge later reduced that award to $87 million."
What Are the Possible Cancer Links to Acetaminophen?
Suspicion of acetaminophen’s carcinogenic potential stems from the fact that it is a major metabolite of phenacetin, a drug connected with cancer more than three decades ago. In 2001, researchers in the International Journal of Cancer wrote:11
"Concern has been raised about the carcinogenic potential of paracetamol (acetaminophen) because it is the major metabolite of phenacetin, which was classified as a human carcinogen by the International Agency for Research on Cancer (IARC) in 1987 and has been withdrawn from the market in most countries …
Because of the established link between phenacetin and malignant tumors of the urinary tract, most epidemiologic studies of paracetamol and cancer have focused on these tumors.
Some of these have reported slightly elevated risks of renal cell cancer or transitional cell cancers of the renal pelvis, ureter or urinary bladder with regular or long-term use of paracetamol, whereas other studies have failed to demonstrate such associations."
Still, the researchers added that they did not find what you would interpret as very strong cancer links with acetaminophen:12
"We found no evidence of an association between use of paracetamol and risk of urinary bladder cancer, but some evidence of an association with upper urinary tract cancers, including cancers of the renal parenchyma, renal pelvis and ureter."
Nearly 20 years later, in January 2020, the Los Angeles Times weighed in on the possible risks and downplayed them, saying the "standards for inclusion" for the Proposition 65 list are so low, even coffee was put on it.13
Acetaminophen Can Cause Liver Damage
As I wrote before, acetaminophen is the top cause of acute liver failure in the U.S. It can even be toxic to your liver at recommended doses when taken daily for just a couple of weeks.14 Part of the reason for the risk is that acetaminophen's recommended dose and the amount of the drug that causes an overdose are very close. There is not much margin of safety.
In fact, studies reveal that taking just a little more acetaminophen than the recommended dose over a few days or weeks (referred to as "staggered overdosing") can be deadlier than one large overdose.15 Research in the Journal of Clinical and Translational Hepatology found:16
"Hepatic injury and subsequent hepatic failure due to both intentional and non-intentional overdose of acetaminophen (APAP) has affected patients for decades, and … it accounts for more than 50% of overdose-related acute liver failure and approximately 20% of the liver transplant cases.
… Although APAP hepatotoxicity follows a predictable timeline of hepatic failure, its clinical presentation might vary. N-acetylcysteine (NAC) therapy is considered as the mainstay therapy, but liver transplantation might represent a life-saving procedure for selected patients."
Acetaminophen Is Linked to Fatal Skin Reactions
Few people have heard of three serious skin reactions linked to acetaminophen, but they are concerning enough that the FDA issued a warning in 2013:17
"Reddening of the skin, rash, blisters, and detachment of the upper surface of the skin can occur with the use of drug products that contain acetaminophen. These reactions can occur with first-time use of acetaminophen or at any time while it is being taken …
Anyone who develops a skin rash or reaction while using acetaminophen or any other pain reliever/fever reducer should stop the drug and seek medical attention right away.”
The three skin conditions that the FDA warns of are very rare but also life-threatening:
Stevens Johnson Syndrome (SJS) — This reaction begins with flu-like symptoms that progress into a painful rash that blisters and causes the top layer of the skin to slough off. This can lead to serious infections, blindness, damage to internal organs, permanent skin damage and death.
Toxic Epidermal Necrolysis (TEN) — TEN also typically begins with flu-like symptoms (cough, headache, aches and fever) and progresses into a blistering rash. Layers of the skin may peel away in sheets and hair and nails may fall out. TENS is often fatal.
Acute Generalized Exanthematous Pustulosis (AGEP) — This skin eruption causes numerous pustules to appear on the skin, often accompanied by fever. This condition typically resolves within two weeks once the acetaminophen is stopped.
No one knows why acetaminophen can cause these extreme skin conditions and there is no way to predict who may be at risk before they take the drug. Even more concerning, as the FDA points out in its warning, the reactions can occur in someone who has safely taken acetaminophen before.
Acetaminophen Not Safe During Pregnancy
Acetaminophen is likely not safe to take for women who are pregnant. A study in JAMA Pediatrics found disturbing links between hyperkinetic disorders (HKD), a severe form of attention-deficit/hyperactivity disorder (ADHD), and ADHD itself.18 The study found a 29% increased risk for ADHD in the children whose mothers had used acetaminophen during pregnancy in the first seven years of their lives and a 37% increased risk of being diagnosed with HKD.19
In a 2015 communication, the FDA cited the JAMA Pediatrics ADHD study. It also cited research that found a possible connection between the use of acetaminophen and other drugs called nonsteroidal anti-inflammatories (NSAIDs) and miscarriage but found the evidence inconclusive.20
The fetal exposure of mothers taking acetaminophen during pregnancy may also increase a child's chances of developing asthma.21 Researchers analyzed data from the Norwegian Mother and Child Cohort Study, which includes many mother/child pairs, and found that prenatal acetaminophen exposure was associated with an increased risk of asthma in offspring.22
Finally, use of acetaminophen during pregnancy may cut levels of testosterone in the womb, negatively affecting males, according to research in mice.23 It's possible that this apparent testosterone reduction interferes with the development of the male reproductive system and explains genital birth defects, infertility and testicular cancer, according to other research.24
In addition to harm to male fetuses, a rat study found that the use of acetaminophen or NSAIDs in pregnancy could reduce the size of ovaries and follicles, and if applied to humans, might indicate that it could affect fertility of resulting daughters and granddaughters.25
Other Acetaminophen Risks
Acetaminophen may not be safe to take when you are drinking alcohol. Research suggests it can greatly increase your risk of kidney dysfunction — even if the amount of alcohol is small.26 Combining alcohol with acetaminophen was found to raise the risk of kidney damage by 123% compared to taking either of them individually.
Besides alcoholics, young adults are particularly at risk of kidney harm as they're more likely to consume both alcohol and acetaminophen.27
Acetaminophen can also affect the immune system. According to a study in Human Vaccines & Immunotherapeutics,28 infants who received acetaminophen right after getting a vaccination experienced lowered immune response and developed significantly fewer antibodies against the disease they were vaccinated against.
Acetaminophen's anti-inflammatory activity might explain the apparent effects by interfering with the body's immune system antibody response, say the researchers.
Other risks that have been associated with the use of acetaminophen include chronic obstructive pulmonary disease (COPD) and reduced lung function, brain damage, increased blood pressure and hearing loss. Finally, acetaminophen may have psychiatric effects, according to research conducted by University of British Columbia researchers in 2016.29
The researchers found that use of acetaminophen may both lessen the ability of people to recognize errors that they make and their concern about whether or not they have made an error.30
Past research has also revealed subtle cognitive effects associated with acetaminophen use, like a 2010 study that indicated acetaminophen may reduce the pain of social rejection.31 Research also showed that acetaminophen had the ability to blunt both positive and negative emotions.32
Regardless of whether acetaminophen is added to California's Proposition 65 as a carcinogen, there are many reasons to avoid this drug when possible and use it cautiously. Further, there are many pain-relieving herbs and practices that you can use to replace acetaminophen for natural relief.