Health, Fitness,Dite plan, health tips,athletic club,crunch fitness,fitness studio,lose weight,fitness world,mens health,aerobic,personal trainer,lifetime fitness,nutrition,workout,fitness first,weight loss,how to lose weight,exercise,24 hour fitness,
Labels
Technology
New Post
[recent][newsticker]
02/01/21
Top Health News -- ScienceDaily
Aging
Alzheimer's
Articles
Articles : Asthma
Articles : CAFO
Articles : Children's Health
Articles : Cholesterol
Articles : Emotional Health
Articles : Fibromyalgia
Articles : GMO
Articles : Heart Health
Articles : Hormones
Articles : Internal Videos
Articles : Interviews
Articles : Men's Health
Articles : Politics
Articles : Thyroid Disease
Articles : Vaccines
Autism
best natural health source
Children's Health
Detoxification
Diabetes
Diet | body+soul
Diet and Weight Loss News -- ScienceDaily
Digestive Diseases
Dite
Dite & weight loss
Drug Industry
Drugs
EFT
EMF
Emotional Health
Finances
fitness
Fitness | body+soul
Fitness/Exercise
Fluoride
Food
Fructose/Sugar
Gardening
Harvard Health Blog
Health
Health | body+soul
Health and Wellness
health news
health tips
Heart Health
information
Joint Support
Juicing
Men's Health
news
Nutrition
Nutrition | body+soul
Pollution
Raw Milk
Soy
Supplements
Swine Flu
Technology
Thyroid Disease
Top Health
Top Health News -- ScienceDaily
Under Armour
Vaccines
Weight Management
women's health
Women's Health News -- ScienceDaily
work place health
Workplace Health News -- ScienceDaily
Amy Schumer’s C-section scar is looking CUTE in her nude selfie
Comedian and actor Amy Schumer has sent the internet into a positive spiral of support and commendation after posting a nude mirror selfie that shows off her 'cute' C-section scar.
from Health | body+soul https://ift.tt/2YyqA7Z
from Health | body+soul https://ift.tt/2YyqA7Z
Prostate drug associated with lower risk of Parkinson's disease
Taking a particular type of medication to treat enlarged prostate is associated with a reduced risk of developing Parkinson's disease, according to a large observational study by researchers at the University of Iowa, and colleagues in Denmark and China. The findings, published in JAMA Neurology, suggest that terazosin, and similar medications, might have potential to prevent or delay the development of Parkinson's disease.
from Top Health News -- ScienceDaily https://ift.tt/2YA6x9l
from Top Health News -- ScienceDaily https://ift.tt/2YA6x9l
Stress on every cell: Mapping the stress axis in detail
Uncovering the activities of the organs, tissues and cells responsible for the body's stress response as they've never before been seen revealed new cells and possible new drug targets.
from Top Health News -- ScienceDaily https://ift.tt/36Azarv
from Top Health News -- ScienceDaily https://ift.tt/36Azarv
New realm of personalized medicine with brain stimulation
Millions of patients suffering from neurological and mental disorders such as depression, addiction, and chronic pain are treatment-resistant. New research paves the way for a promising alternative: personalized deep brain stimulation. Researchers have found a way to predict what effect electrical stimulation will have on an individual's brain activity across multiple brain regions. The work represents a major step forward in achieving new therapies for a whole host of neurological and mental disorders.
from Top Health News -- ScienceDaily https://ift.tt/3pJg7mq
from Top Health News -- ScienceDaily https://ift.tt/3pJg7mq
Lactobacillus manipulates bile acids to create favorable gut environment
Probiotic Lactobacillus bacteria use enzymes situationally to manipulate bile acids and promote their own survival in the gut.
from Top Health News -- ScienceDaily https://ift.tt/3j7xxqd
from Top Health News -- ScienceDaily https://ift.tt/3j7xxqd
Potential therapeutic targets to inhibit colorectal cancer progression
Researchers have revealed that colorectal cancer tissues contain at least two types of fibroblasts, namely, cancer-promoting fibroblasts and cancer-restraining fibroblasts, and that the balance between them is largely involved in the progression of colorectal cancer. Their findings suggest that artificially altering the balance between the two types of cells could curb the spread of colorectal cancer tumors, which may become an effective strategy for preventing cancer progression.
from Top Health News -- ScienceDaily https://ift.tt/3j86jzK
from Top Health News -- ScienceDaily https://ift.tt/3j86jzK
The ‘Sex and the City’ reboot will make COVID references and ugh
Pretty much the one thing we didn't want from the Sex and the City reboot, as revealed by Sarah Jessica Parker.
from Health | body+soul https://ift.tt/3avi27M
from Health | body+soul https://ift.tt/3avi27M
Use of pronouns may show signs of an impending breakup
Evidence of an impending breakup may exist in the small words used in everyday conversations months before either partner realizes where their relationship is heading, according to new psychology research.
from Top Health News -- ScienceDaily https://ift.tt/3oAcCgJ
from Top Health News -- ScienceDaily https://ift.tt/3oAcCgJ
Wonder fungi in goat's gut
From biofuels and other commodity chemicals to methane production, genomic study peers into the mysteries of a goat's gut.
from Top Health News -- ScienceDaily https://ift.tt/2YztGsz
from Top Health News -- ScienceDaily https://ift.tt/2YztGsz
Detecting fake news designed to manipulate stock markets
Social media is increasingly used to spread fake news. The same problem can be found on the capital market - criminals spread fake news about companies in order to manipulate share prices. Researchers have developed an approach that can recognize such fake news, even when the news contents are repeatedly adapted.
from Top Health News -- ScienceDaily https://ift.tt/39Bk1rE
from Top Health News -- ScienceDaily https://ift.tt/39Bk1rE
Nutrition, companionship reduce pain in mice with sickle cell disease
Researchers have found that an enriched diet and companionship can reduce pain in mice with sickle cell disease by increasing serotonin. They also discovered that duloxetine, an antidepressant that boosts serotonin levels, could be an alternative to opioids in treating chronic pain.
from Top Health News -- ScienceDaily https://ift.tt/2LdqWy2
from Top Health News -- ScienceDaily https://ift.tt/2LdqWy2
Breakthrough in mobile determination of QT prolongation
Researchers have been using artificial intelligence (AI) to develop a mobile device that can identify certain patients at risk of sudden cardiac death.
from Top Health News -- ScienceDaily https://ift.tt/3cspVgN
from Top Health News -- ScienceDaily https://ift.tt/3cspVgN
Larger panel finds more gene mutations, treatment targets for leukemia
A gene panel that looks for about 10 times the number of cancer-causing genes as panels currently used to diagnose and fine tune treatment for a variety of cancers is effective at identifying problematic genes in the most common leukemia, investigators report.
from Top Health News -- ScienceDaily https://ift.tt/2YAFniQ
from Top Health News -- ScienceDaily https://ift.tt/2YAFniQ
Glitch in genome architecture may cause B-cell malignancies
Restoring an enzyme that maintains the way chromosomes are packed inside cells may lead to new therapies for some blood cancers, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/3alkVba
from Top Health News -- ScienceDaily https://ift.tt/3alkVba
Wearable sensor monitors health, administers drugs using saliva and tears
A new kind of wearable health device would deliver real-time medical data to those with eye or mouth diseases.
from Top Health News -- ScienceDaily https://ift.tt/2Mq8mTJ
from Top Health News -- ScienceDaily https://ift.tt/2Mq8mTJ
Toxin-antitoxin function fuels antibiotic-resistance research
Toxin-antitoxin (TA) systems are now known to negatively control plasmid replication.
from Top Health News -- ScienceDaily https://ift.tt/3pD6K7y
from Top Health News -- ScienceDaily https://ift.tt/3pD6K7y
Don't let pressure of one-upmanship dictate your gift selection
Researchers set out to understand gift giving dynamics in these settings and how a giver's and a recipient's evaluation of the giver's gift is influenced by the other gifts the recipient receives.
from Top Health News -- ScienceDaily https://ift.tt/3pIw38k
from Top Health News -- ScienceDaily https://ift.tt/3pIw38k
Hyaluronan is effective in treating chronic lung disease
Researchers found that inhaling unfragmented hyaluronan improves lung function in patients suffering from severe exacerbation of chronic obstructive pulmonary disease (COPD). Hyaluronan, a sugar secreted by living tissue that acts as a scaffold for cells, is also used in cosmetics as a skin moisturizer and as a nasal spray to moisturize lung airways. Utilized as a treatment, hyaluronan decreased the number of days in the hospital.
from Top Health News -- ScienceDaily https://ift.tt/3oD3at0
from Top Health News -- ScienceDaily https://ift.tt/3oD3at0
Your toothbrush reflects you, not your toilet
After studying microbial communities living on bristles from used toothbrushes, researchers found those communities matched microbes commonly found inside the mouth and on skin.
from Top Health News -- ScienceDaily https://ift.tt/3ra2BZ3
from Top Health News -- ScienceDaily https://ift.tt/3ra2BZ3
Origami with DNA
To study the behavior of T-cells, an unusual method was used: DNA molecules were folded in an ingenious way, similar to the paper folding art origami. In this way, not just a double helix is created, but a rectangular 'molecular raft' that floats across a cell membrane and serves as a tool for novel measurements.
from Top Health News -- ScienceDaily https://ift.tt/39AmrqE
from Top Health News -- ScienceDaily https://ift.tt/39AmrqE
Supersaturation: The barrier between protein folding and misfolding
It's commonly accepted that protein folding/misfolding are alternative reactions of unfolded proteins but the principles governing this remain unknown. Here, researchers describe a general concept that links protein folding and misfolding: protein folding and amyloid formation are separated by the supersaturation barrier of a denatured protein. Breakdown of this supersaturation barrier is required to shift the protein to the amyloid pathway, linking Anfinsen's intramolecular folding universe with the 'outer' intermolecular misfolding universe.
from Top Health News -- ScienceDaily https://ift.tt/36u78hm
from Top Health News -- ScienceDaily https://ift.tt/36u78hm
Bleeding gums may be a sign you need more vitamin C in your diet
Bleeding of the gums on gentle probing, or gingival bleeding tendency, and also bleeding in the eye, or retinal hemorrhaging, were associated with low vitamin C levels in the bloodstream.
from Top Health News -- ScienceDaily https://ift.tt/3thW28U
from Top Health News -- ScienceDaily https://ift.tt/3thW28U
Inherited immune condition reversed by random DNA change
Researchers have revealed how a rare DNA change rebalanced the immune system of patients with a life-threatening genetic immunodeficiency.
from Top Health News -- ScienceDaily https://ift.tt/39Cnc2w
from Top Health News -- ScienceDaily https://ift.tt/39Cnc2w
Why do psychiatric drugs help some, but not others? Study offers clues
New research shows that a key protein in the brain called AKT may function differently in males than females. The study also offers a closer look at where, precisely, in the brain things may go wrong with it, marking an important step toward more targeted and less harmful therapies.
from Top Health News -- ScienceDaily https://ift.tt/3tfGeDx
from Top Health News -- ScienceDaily https://ift.tt/3tfGeDx
Temperature Scans Are Unreliable in Detecting COVID
An early sign of many infections is a fever or an increase in your core temperature that your body uses to help fight pathogens. Researchers have found the no-contact forehead thermometers commonly used to screen for fever in public places are an ineffective and unreliable means of detecting COVID-19.1
Thermoregulation is an important part of maintaining a homeostatic environment in the body. Homeostasis is a physiological state in which an organism seeks stability or equilibrium between interdependent systems. Your body temperature is integral to creating equilibrium for other systems to optimally function. The entire system is complex and sometimes may seem counterintuitive.2
Your body can use negative and positive feedback loops3 to help regulate your core temperature within a narrow range, irrespective of the external environment.4 Infection is another reason your body's core temperature can rise. The primary virus of interest in 2020 has been SARS-CoV-2 that triggers COVID-19 infection.
The first confirmed case in the U.S. occurred January 21, 2020, when the Centers for Disease Control and Prevention found a Washington state resident who had recently returned from Wuhan, China, was infected.5 By January 23, 2020, Wuhan was under quarantine and shortly thereafter the U.S. declared a public health emergency.
The early unfolding events of the COVID-19 pandemic included recommended measures to help reduce the spread of an unknown virus. These included social distancing, sheltering in place, mask-wearing and temperature taking.
Skin Temperature Can Change Independent of Core Temperature
The body maintains an internal temperature that varies less than 1.8 degrees Fahrenheit (1 degree Celsius) throughout the day, depending on your physical activity, foods you've eaten or emotional state.6
A change in core body temperature outside this range can happen during an illness or when the conditions in the external environment are more than your body is able to handle, such as extreme heat or extreme cold. In high heat, the body will shunt blood to the skin to increase sweat production and release heat, which assists in thermoregulation.
This variability in skin temperature independent of your core body temperature is one reason the no-contact forehead scanners are unreliable. While fever is a common symptom of COVID-19, the scanners can result in false negatives and false positives.
Researchers in physiology are suggesting that using the same scanners to assess a person's temperature at the fingertip and eye would offer more reliable readings.7 The study was published in Experimental Physiology and co-led by physiologist and expert in thermoregulation, Michael J. Tipton, Ph.D., who is also editor-in-chief of the same journal.8
While reviewing the science behind temperature taking, the writers suggested infrared thermography forehead scanners were of limited use for mass screening.9 As outlined in a press release from the Physiological Society, the paper determined four key factors that relate to using the scanners:10
- Not all people who have the virus have a fever, so temperature alone is not a good indicator.
- Skin temperature can vary from body core temperature and therefore is not an accurate estimate, and a direct measure of core temperature is impractical.
- Not every person with a fever, even an accurate core body temperature, has COVID-19.
- Using temperature assessments from the finger and the eye may offer more reliable information of an increase in body core temperature.
Tipton Proposes Adapting Infrared Thermography Scanners
In their review of early data, the researchers found the most common symptom in 55,924 patients with confirmed cases who presented in China through February 22, 2020, was fever. In this group, at least 11% did not have a fever and fewer than half with suspected disease who were admitted to the hospital had a fever.11
The press release cites a 2005 study in which forehead temperatures were compared across three infrared forehead thermometers in 1,000 participants. The measurements varied by as much as 3.6 degrees F (2 degrees C).
In another study with 500 participants, more than 80% of the infrared measurements produced a false negative result. There is a range of reasons that thermometers can produce false-negative results, including:12
|
Exercise |
Sunburn |
|
Alcohol |
Cancer |
|
Blood pressure |
Ambient temperature |
|
Adipose levels in the body |
Distance from the scanner |
Tipton commented on the results of the study and how the information could be used, saying:
“If scanners are not giving an accurate reading, we run the risk of falsely excluding people from places they may want, or need, to go, and we also risk allowing people with the virus to spread the undetected infection they have. Using a surface temperature scanner to obtain a single surface temperature, usually the forehead, is an unreliable method to detect the fever associated with COVID-19.
Too many factors make the measurement of a skin temperature a poor surrogate for deep body temperature; skin temperature can change independently of deep body temperature for lots of reasons. Even if such a single measure did reflect deep body temperature reliably, other things, such as exercise can raise deep body temperature.
We think we can improve the identification of the presence of fever using the same kit but looking at the difference between eye and finger temperature – it’s not perfect, but it is potentially better and more reliable.”
Not All People With COVID-19 Have a Fever
As Tipton pointed out from data gathered early in the pandemic through February 2020, not all people who have COVID-19 will have a fever. As more data have been gathered throughout 2020, the number of people who may have an infection, but present without fever, has grown. Your body produces a fever with infection since most viruses and bacteria find it harder to survive in higher temperatures.13
As with other types of infection, people may experience a range of mild to severe disease. The CDC lists several symptoms associated with COVID-19 that may appear within two to 14 days after being exposed to SARS-CoV-2. Among these are fever, cough, shortness of breath, fatigue and a new loss of taste or smell.14
The difference in the symptoms a person may experience is also related to whether they have a mild, moderate or severe infection. To date, there has not been a definitive study on the prevalence of individuals with COVID-19 who will also present with a fever.
Research published in the Journal of the American Medical Association offers a clue that a fever is not as common with mild illness as was originally believed.15 The researchers evaluated the symptoms of 202 participants who completed the study. They found that an alteration in taste or smell was one of the first symptoms reported in patients who had mild or asymptomatic disease.
They cautioned that the sample was geographically limited and patients with severe disease were not included. A second later study from South Korea showed in 213 people with confirmed cases of COVID-19, the most common symptom was a cough followed by a loss of taste and smell.16 In this group, fever was only recorded in 11.6% of the individuals.
Normal Temperatures Have Dropped Below 98.6
German doctor Carl Reinhold August Wunderlich collected data from 2,500 people, amounting to millions of temperatures.17 Whether people were sick or healthy, he recorded their body temperatures and then analyzed and published the data in the mid-1800s. This data helped establish a normal temperature of 98.6 Fahrenheit (37 Celsius), which medicine uses as one factor in a health evaluation.
However, research published in 2020 found that human core body temperatures in the U.S. have been declining through the Industrial Revolution.18 Dr. Julie Parsonnet from Stanford University department of medicine and her team gathered more than 677,000 temperature measurements from nearly 190,000 people collected from 1862 to 2017.
The data were split into three chronological groups and analyzed, leading the team to conclude that body temperatures have dropped an average of 1.06 F in men and 0.58 F in women over a 200-year time period.19 To minimize potential measurement bias, the scientists also compared temperature readings within a specific population. Commenting on the results of the study, Parsonnet said:20
“Our temperature’s not what people think it is. What everybody grew up learning, which is that our normal temperature is 98.6, is wrong. Physiologically, we’re just different from what we were in the past.
The environment that we’re living in has changed, including the temperature in our homes, our contact with microorganisms and the food that we have access to. All these things mean that although we think of human beings as if we’re monomorphic and have been the same for all of human evolution, we’re not the same. We’re actually changing physiologically.”
While the results are interesting, Kenneth Welch, Ph.D., who was not involved in the study, believes it will not make a difference in the day-to-day life of individuals.21 Even infections that trigger a small rise in body temperature normally also trigger body aches, chills or headaches commonly associated with a fever. Rising temperatures from other environmental factors or even allergies do not usually trigger the same experience.
How to Take an Accurate Temperature
When you have a cold, flu or other infectious condition, such as COVID-19, it is always best to steer clear of others and reduce the spread of infection. After all, no one really enjoys being sick.
Other than body aches, chills and generally feeling miserable, you have several options for determining if you have a fever at home.22 A digital thermometer can be used in the mouth, rectum or under the arm. Purchase disposable protective sleeves to help keep the thermometer clean and make sure you're not passing germs from one person to another.
If you plan to use both oral and rectal temperatures, use separate thermometers for each and be sure they're labeled accordingly. When taking an oral temperature, wait at least 15 minutes after you've eaten or drunk anything to avoid an inaccurate reading.
A tympanic (ear) thermometer takes a digital reading from inside the ear canal and must be positioned correctly to get an accurate reading. Ear wax and small ear canals can interfere with accuracy. To use an infrared scanner, the thermometer must be placed over the temporal artery to get an accurate reading.
The type of thermometer you choose may not be as important as following the directions to achieve an accurate measurement and ensure you don't pass germs with each use. It is crucial you do not rely strictly on temperature to determine the severity of an illness. Additional symptoms, such as dehydration, lethargy and confusion, are strong indicators of illness and must be considered.
from Articles https://ift.tt/3cuBWC8
via IFTTT
Journal of Medicine Says HCQ + Zinc Reduces COVID Deaths
Early on in the COVID-19 pandemic, doctors around the world reported high success rates using an inexpensive treatment protocol of hydroxychloroquine (HCQ) and zinc, typically in combination with an antibiotic to treat secondary bacterial infections.
Almost immediately, government health agencies and mainstream media started attacking the treatment, going so far as to ban the prescription and use of HCQ for COVID-19 in some areas. Over time, it became painfully clear that a concerted and coordinated effort to prevent its use was afoot.
One of the most obvious reasons for why certain individuals and companies might want to prevent the use of an inexpensive generic drug is because it might eliminate the need for a vaccine or other antiviral medication under development.1 Hundreds of millions of dollars have been invested, and drug companies were, and still are, counting on a massive payday. As noted by Dr. Meryl Nass in a June 27, 2020, blog post:2
“Hydroxychloroquine has been used safely for 65 years in many millions of patients. And so the message was crafted that the drug is safe for its other uses, but dangerous when used for COVID-19. It doesn’t make sense, but it seems to have worked. Were these acts carefully orchestrated? …
Might these events have been planned to keep the pandemic going? To sell expensive drugs and vaccines to a captive population? Could these acts result in prolonged economic and social hardship, eventually transferring wealth from the middle class to the very rich?”
Politicizing Medicine Has Grave Consequences
The fight over HCQ also appears to have had political underpinnings, and by politicizing medicine, the media has played a role that can readily be likened to agents of genocide. There’s no telling how many lives may have been saved had they done their due diligence and reported the science truthfully.
Most of us in the holistic field have been aware that the intent of censorship is to mislead people. After all, a majority of news outlets rely on revenue from advertisers, and drug companies tend to spend the most. As a result, what the drug industry wants is what the media deliver.
During this pandemic, conventional doctors have gotten a taste of what it’s like as well and, clearly, many have been absolutely floored by it. It’s certainly understandable, because to censor potentially lifesaving medical treatment during a global pandemic really brings it to a whole new level of evil.
As just one example among many, July 23, 2020, Dr. Harvey A. Risch, professor of epidemiology at Yale School of Public Health, published an op-ed in Newsweek in which he expressed his dismay and frustration:3
“I have authored over 300 peer-reviewed publications and currently hold senior positions on the editorial boards of several leading journals.
I am usually accustomed to advocating for positions within the mainstream of medicine, so have been flummoxed to find that, in the midst of a crisis, I am fighting for a treatment that the data fully support but which, for reasons having nothing to do with a correct understanding of the science, has been pushed to the sidelines.
As a result, tens of thousands of patients with COVID-19 are dying unnecessarily … I am referring, of course, to the medication hydroxychloroquine.
When this inexpensive oral medication is given very early in the course of illness, before the virus has had time to multiply beyond control, it has shown to be highly effective, especially when given in combination with the antibiotics azithromycin or doxycycline and the nutritional supplement zinc.”
In what appears to be an effort to change the tide, a medical review4 in the January 2021 issue of The American Journal of Medicine now urges early use of HCQ and zinc. The authors include Risch, as well as a long list of medical doctors from hospitals around the world.
The Importance of Early Outpatient Treatment
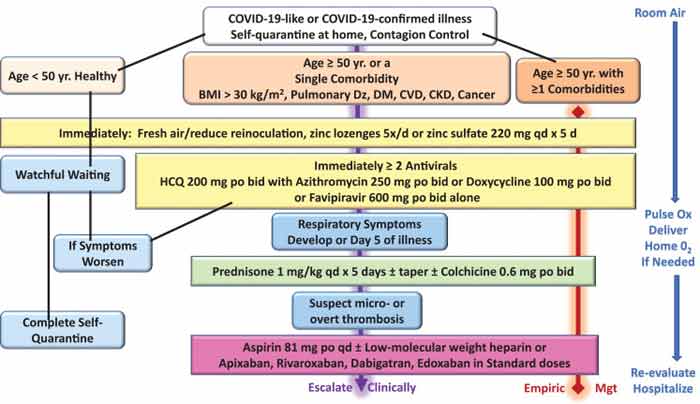
Risch’s paper, “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection,” points out that:5
“In the absence of clinical trial results, physicians must use what has been learned about the pathophysiology of SARS-CoV-2 infection in determining early outpatient treatment of the illness with the aim of preventing hospitalization or death …
Therapeutic approaches based on these principles include 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, 4) antiplatelet/antithrombotic therapy, and 5) administration of oxygen, monitoring, and telemedicine.”
The authors stress that “Most patients who arrive to the hospital … with COVID-19 do not initially require forms of advanced medical care,” and that, therefore, “it is conceivable that some, if not a majority, of hospitalizations could be avoided with a treat-at-home first approach.”
They also stress that since it can take up to a week to get PCR test results back, it’s important to start treatment before results are known. “For patients with cardinal features of the syndrome (i.e., fever, body aches, nasal congestion, loss of taste and smell, etc.) … treatment can be the same as those with confirmed COVID-19,” they say.
The Case for HCQ and Zinc
In terms of early drug treatment for patients who are quarantining at home, the authors recommend using a combination of HCQ and zinc lozenges, along with several other drugs (depending on your symptoms).
While I will review those here, keep in mind that I do not necessarily recommend using all of them, as in some cases there are safer alternatives. At the end of this article, I will summarize my personal at-home treatment recommendation, which I believe is among the absolute safest and most effective.
That said, in his paper, Risch and his co-authors explain the rationale for using HCQ and zinc as follows:6
“Hydroxychloroquine (HCQ) is an antimalarial/anti-inflammatory drug that impairs endosomal transfer of virions within human cells. HCQ is also a zinc ionophore that conveys zinc intracellularly to block the SARS-CoV-2 RNA-dependent RNA polymerase, which is the core enzyme of the virus replication.
The currently completed retrospective studies and randomized trials have generally shown these findings:
1. when started late in the hospital course and for short durations of time, antimalarials appear to be ineffective
2. when started earlier in the hospital course, for progressively longer durations and in outpatients, antimalarials may reduce the progression of disease, prevent hospitalization, and are associated with reduced mortality …
A typical HCQ regimen is 200 mg bid for 5 days and extended to 30 days for continued symptoms. A minimal sufficient dose of HCQ should be used, because in excessive doses the drug can interfere with early immune response to the virus ...
Zinc is a known inhibitor of coronavirus replication … This readily available nontoxic therapy could be deployed at the first signs of COVID-19. Zinc lozenges can be administered 5 times a day for up to 5 days and extended if needed if symptoms persist.
The amount of elemental zinc lozenges is <25% of that in a single 220-mg zinc sulfate daily tablet. This dose of zinc sulfate has been effectively used in combination with antimalarials in early treatment of high-risk outpatients with COVID-19.”
It’s worth noting that in areas where hydroxychloroquine is hard to get a hold of, the nutritional supplement quercetin may be a useful (and perhaps even better) substitute, as its primary mechanism of action is identical to that of the drug. It also has antiviral activity of its own.
You can learn more about this in “Is Quercetin a Safer Alternative to Hydroxychloroquine?” “Quercetin Boosts Interferon Response to Viruses and COVID-19” and “How to Improve Zinc Uptake with Quercetin to Boost Immune Health.”
Zinc Is a Crucial Key
While much attention is placed on HCQ, it in and of itself is not the answer. Zinc is. Both HCQ and quercetin are zinc ionophores, meaning they shuttle zinc into the cell,7,8 and there’s compelling evidence to suggest the primary benefit of the HCQ protocol actually comes from the zinc, which effectively inhibits viral replication.9
If given early, zinc along with a zinc ionophore should, at least theoretically, help lower the viral load and prevent the immune system from becoming overloaded. The problem is that zinc does not readily enter cells, which is why a zinc ionophore is needed.
Evidence of this was presented in a September 2020 study10 in the Journal of Medical Microbiology. In it, they compared outcomes in hospitalized COVID-19 patients treated with one of three regimens: HCQ alone, Azithromycin alone, or a triplet regimen of hydroxychloroquine, azithromycin and zinc.
While the addition of zinc had no impact on the length of hospitalization, ICU duration or duration of ventilation, univariate analyses showed it did:
- Increase hospital discharge frequency
- Decrease the need for ventilation
- Decrease ICU admission rates
- Decrease the rate of transfer to hospice for patients who were never admitted to the ICU
- Decrease mortality
As noted by the authors:11
“After adjusting for the time at which zinc sulfate was added to our protocol, an increased frequency of being discharged home (OR 1.53 …) reduction in mortality or transfer to hospice remained significant (OR 0.449 …). This study provides the first in vivo evidence that zinc sulfate in combination with hydroxychloroquine may play a role in therapeutic management for COVID-19.”
Another paper that addressed the crucial role of zinc was published in the September 2020 issue of Medical Hypotheses:12
“Besides direct antiviral effects, CQ/HCQ [chloroquine and/or hydroxychloroquine] specifically target extracellular zinc to intracellular lysosomes where it interferes with RNA-dependent RNA polymerase activity and coronavirus replication.
As zinc deficiency frequently occurs in elderly patients and in those with cardiovascular disease, chronic pulmonary disease, or diabetes, we hypothesize that CQ/HCQ plus zinc supplementation may be more effective in reducing COVID-19 morbidity and mortality than CQ or HCQ in monotherapy. Therefore, CQ/HCQ in combination with zinc should be considered as additional study arm for COVID-19 clinical trials.”
Antibiotics, Steroids and Other Treatment Additions
In addition to HCQ and zinc, Risch13 et.al also recommend using one of two antibiotics — azithromycin or doxycycline — primarily to address secondary bacterial infections. Azithromycin also has antiviral properties and anti-inflammatory effects, while doxycycline has “multiple intracellular effects that may reduce viral replication, cellular damage, and expression of inflammatory factors.”
According to the authors, COVID-19 studies that used azithromycin found “markedly reduced durations of viral shedding, fewer hospitalizations, and reduced mortality combination with HCQ.”
People with known or suspected arrhythmias, and anyone taking a contraindicated medication, should get a thorough workup and review of baseline electrocardiogram though before receiving HCQ and/or azithromycin. In those worried about azithromycin’s effects on the heart, doxycycline is a better alternative as it has no ill effects on your heart. On the downside, it can cause gastrointestinal upset and esophagitis instead.
An important side note here is that while not addressed in this paper, all antibiotics have the drawback of disrupting your gut microbiome, and should therefore be used only if absolutely needed.
Risch14 et.al also recommend using corticosteroids, which have immunomodulating effects and help reduce the effects of cytokine storms. As explained in their paper:
“In COVID-19, some of the first respiratory findings are nasal congestion, cough, and wheezing. These features are due to excess inflammation and cytokine activation.
Early use of corticosteroids is a rational intervention for patients with COVID-19 with these features as they would be in acute asthma or reactive airways disease … One potential dosing scheme for outpatients starting on day 5 or the onset of respiratory symptoms is prednisone 1 mg/kg given daily for 5 days with or without a subsequent taper.”
Other treatment additions include:
- Colchicine, a nonsteroidal antimitotic that has been shown to reduce D-dimer levels and improve outcomes in hospitalized COVID-19 patients
- Antiplatelet agents such as aspirin (81 mg daily) or heparin to treat the abnormal blood clotting sometimes seen in COVID-19
- Supplemental oxygen if needed
To reduce the risk of self-reinoculation (since the virus is airborne), they also recommend opening windows and/or spending long periods of time outdoors (away from others) without a face covering.
The figure below, from The American Journal of Medicine and republished in Science Direct,15 illustrates the different approaches to home care suggested depending on whether you are healthy, have a single comorbidity or several, and at which point in the disease process the various drugs should be administered.
Hydroxychloroquine Has a Proven Safety Profile
While media headlines have painted HCQ as a life-threatening drug, it actually has a very robust safety profile that goes back decades. In a paper published in the American Journal of Epidemiology,16 Risch reviewed several large-scale studies demonstrating the safety of the medication.
In his Newsweek article,17 he also pointed out that the adverse event reports cited by the U.S. Food and Drug Administration when it warned HCQ might cause cardiac arrhythmia, especially when administered with azithromycin, were from patients who had used HCQ for very long periods of time for the treatment of chronic conditions such as lupus or rheumatoid arthritis. The same risks simply do not apply when you’re taking HCQ for a few days or weeks.
“Even if the true rates of arrhythmia are tenfold higher than those reported, the harms would be minuscule compared to the mortality occurring right now in inadequately treated high-risk COVID-19 patients,” Risch wrote.18
“This fact is proven by an Oxford University study of more than 320,000 older patients taking both hydroxychloroquine and azithromycin, who had arrhythmia excess death rates of less than 9/100,000 users … A new paper in the American Journal of Medicine by established cardiologists around the world fully agrees with this.”
Indeed, the so-called evidence that HCQ causes lethal heart problems has been shown to be fraudulent. One study was retracted after it was discovered the data had been manufactured, and other large-scale trials were all using toxic doses.
While doctors reporting success with the drug were using standard doses around 200 mg per day for either a few days or maybe a couple of weeks, studies such as the Bill & Melinda Gates-funded19 Recovery Trial used 2,400 mg of hydroxychloroquine during the first 24 hours — three to six times higher than the daily dosage recommended20 — followed by 400 mg every 12 hours for nine more days for a cumulative dose of 9,200 mg over 10 days.
Similarly, the Solidarity Trial,21 led by the World Health Organization, used 2,000 mg on the first day, and a cumulative dose of 8,800 mg over 10 days. These doses are simply too high.
Meanwhile, a July 1, 2020, retrospective analysis22,23,24 of 2,541 patients in Michigan found use of hydroxychloroquine alone cut mortality by more than half, from 26.4% to 13.5%. Patients received 400 mg of hydroxychloroquine twice on day 1, followed by 200 mg twice a day for the next four days.
No adverse heart-related events were observed. Hydroxychloroquine in combination with azithromycin had a mortality rate of 20.1%, and azithromycin alone had a mortality rate of 22.4%. The azithromycin was dosed as 500 mg on day 1, followed by 250 mg once a day for the next four days.
According to the authors,25 “The combination of hydroxychloroquine + azithromycin was reserved for selected patients with severe COVID-19 and with minimal cardiac risk factors.” Unfortunately, zinc was not included in this trial.
“Physicians who have been using these medications in the face of widespread skepticism have been truly heroic,” Risch wrote in Newsweek.26 “They have done what the science shows is best for their patients, often at great personal risk.
I myself know of two doctors who have saved the lives of hundreds of patients with these medications, but are now fighting state medical boards to save their licenses and reputations. The cases against them are completely without scientific merit …
As all know, the medication has become highly politicized. For many, it is viewed as a marker of political identity, on both sides of the political spectrum. Nobody needs me to remind them that this is not how medicine should proceed … Reality demands a clear, scientific eye on the evidence and where it points”
With that in mind, evidence that HCQ could be useful against SARS-CoV-2 goes as far back as 2005, when the article “Chloroquine Is a Potent Inhibitor of SARS Coronavirus Infection and Spread” was published in the Virology Journal.27
Did Dr. Anthony Fauci, appointed to lead the White House Pandemic Response Team, know about this? One could argue he should have. And, if he did, why didn’t he say something? According to this study:28
“… chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage.”
In other words, chloroquine functioned as both a prophylactic (prevention) and a treatment against SARS coronavirus. This is precisely what many doctors have found with HCQ as well — a drug that is very similar to chloroquine but has a safer profile — when used against SARS-CoV-2.
Nebulized Peroxide — My Favorite Treatment Choice
While HCQ with zinc appears to be a very useful early treatment choice, my personal choice for the treatment of COVID-19 symptoms is nebulized peroxide. This is a home remedy I recommend everyone familiarize themselves with, as in many cases it can improve symptoms in mere hours. You can also use it as a preventive strategy if you know you’ve been exposed to someone who is ill.
Nebulizing hydrogen peroxide into your sinuses, throat and lungs is a simple, straightforward way to augment your body’s natural expression of hydrogen peroxide to combat infections and can be used both prophylactically after known exposure to COVID-19 and as a treatment for mild, moderate and even severe illness.
Dr. David Brownstein, who has successfully treated over 100 COVID-19 patients with nebulized peroxide, published a case paper29 about this treatment in the July 2020 issue of Science, Public Health Policy and The Law. He also reviews its benefits in “How Nebulized Peroxide Helps Against Respiratory Infections.”
Nebulized hydrogen peroxide is extremely safe, and all you need is a desktop nebulizer and food-grade hydrogen peroxide, which you’ll need to dilute with saline to 0.1% strength. I recommend buying these items beforehand so that you have everything you need and can begin treatment at home at the first signs of a respiratory infection.
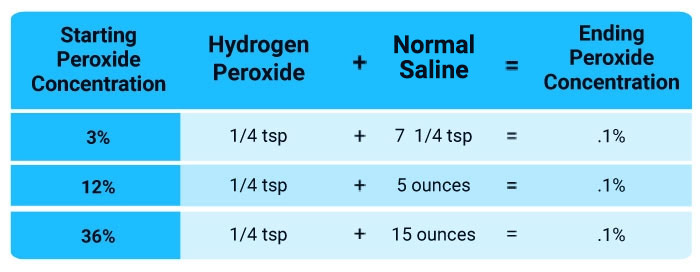
In the video above, I go over the basics of this treatment. Be sure to buy a nebulizer that plugs into an electrical outlet, as battery-driven ones are too low-powered to be truly effective. Also make sure your nebulizer comes with a face mask, not just a mouth piece. If it doesn’t come with a face mask, you can pick one up separately. Just search Amazon for “nebulizer face mask for adults.”
from Articles https://ift.tt/39Bf9mz
via IFTTT
Weekly Health Quiz: Mask, Censorship and COVID
1 Which of the following appears to be a useful treatment at all stages of SARS-CoV-2 infection, but works best as a prophylactic?
- Resveratrol
- Aspirin
- Ivermectin
While preliminary evidence seems to suggest ivermectin can be useful at all stages of SARS-CoV-2 infection, its real strength appears to be prophylactic. Of 58 health care workers who took ivermectin once a month for four months, only four were diagnosed with COVID-19, compared to 44 of the 60 who declined the medication. Learn more.
- Steroids
2 Studies have warned COVID-19 vaccines may result in more serious disease when exposed to the virus by way of:
- Toxic exposure
- Tricking body into shutting down autophagy
- Making your body produce live virus internally
- Pathogenic priming and immune enhancement
Studies have warned COVID-19 vaccines may result in more serious disease when exposed to the virus, either through antibody-dependent immune enhancement or pathogen priming that triggers an autoimmune response. Learn more.
3 Living in the "fog of war" can have a number of ill effects, including:
- Clouding your judgment as you try to make decisions
The "fog of war" is a term used to describe the uncertainty, chaos and confusion that can occur during battle. What you thought was true entering into the battle may be turned upside down, clouding your judgment as you try to make decisions in a sort of suspended reality. Learn more.
- Exposing you to air pollutants
- Blocking your body's production of vitamin D
- Making you feel sleepy
4 Wearing two masks instead of one may potentially lower the risk of viruses entering your airway by subjecting them to an obstacle course of material, but it also poses a risk of:
- Looking funny
- Making it too hard to breathe
There's just one pesky problem. "At some point, 'we run the risk of making it too hard to breathe,' she said." If you can get past that trade-off, the rationale seems to be that if you add enough layers of material, infectious droplets must travel through an obstacle course of sorts, and eventually you'll stop something from getting through. Learn more.
- Creating more laundry
- Not fitting correctly on your face
5 By censoring social media posts or banning a user from its platforms, Big Tech can effectively:
- Ensure the continuation of free speech
- Protect public health
- Support or dismantle certain agendas
Regardless of one's political affiliations, the move highlights the immense control that corporations have over online information and how it can be yielded to support, or dismantle, certain agendas. Learn more.
- Stop conspiracy theorists
6 Many commonly reported side effects from the COVID-19 gene therapy "vaccines," such as dyskinesia (impairment of voluntary movement), ataxia (lack of muscle control) and intermittent or chronic seizures, appear to be caused by which of the following?
- Viral infection
- Bacterial infection
- Breakdown of neurons
- Brain inflammation
Many commonly reported side effects from the COVID-19 gene therapy "vaccines" appear to be caused by brain inflammation. Learn more.
from Articles https://ift.tt/3j2akpq
via IFTTT
MKRdezign
Powered by Blogger.