Health, Fitness,Dite plan, health tips,athletic club,crunch fitness,fitness studio,lose weight,fitness world,mens health,aerobic,personal trainer,lifetime fitness,nutrition,workout,fitness first,weight loss,how to lose weight,exercise,24 hour fitness,
Labels
Technology
New Post
[recent][newsticker]
12/28/20
Top Health News -- ScienceDaily
Aging
Alzheimer's
Articles
Articles : Asthma
Articles : CAFO
Articles : Children's Health
Articles : Cholesterol
Articles : Emotional Health
Articles : Fibromyalgia
Articles : GMO
Articles : Heart Health
Articles : Hormones
Articles : Internal Videos
Articles : Interviews
Articles : Men's Health
Articles : Politics
Articles : Thyroid Disease
Articles : Vaccines
Autism
best natural health source
Children's Health
Detoxification
Diabetes
Diet | body+soul
Diet and Weight Loss News -- ScienceDaily
Digestive Diseases
Dite
Dite & weight loss
Drug Industry
Drugs
EFT
EMF
Emotional Health
Finances
fitness
Fitness | body+soul
Fitness/Exercise
Fluoride
Food
Fructose/Sugar
Gardening
Harvard Health Blog
Health
Health | body+soul
Health and Wellness
health news
health tips
Heart Health
information
Joint Support
Juicing
Men's Health
news
Nutrition
Nutrition | body+soul
Pollution
Raw Milk
Soy
Supplements
Swine Flu
Technology
Thyroid Disease
Top Health
Top Health News -- ScienceDaily
Under Armour
Vaccines
Weight Management
women's health
Women's Health News -- ScienceDaily
work place health
Workplace Health News -- ScienceDaily
Discovery about how cancer cells evade immune defenses inspires new treatment approach
Researchers have learned how chromosomal instability allows cancer cells to avoid immune defenses and metastasize (spread). The discovery opens up potential new avenues for treatment.
from Top Health News -- ScienceDaily https://ift.tt/3pxGtHc
from Top Health News -- ScienceDaily https://ift.tt/3pxGtHc
Vaping could cloud your thoughts, new studies suggest
Both adults and kids who vape were more likely to report difficulty concentrating, remembering, or making decisions than their non-vaping, non-smoking peers on two annual national surveys. Survey results also suggest that kids were more likely to experience mental fog if they started vaping before the age of 14.
from Top Health News -- ScienceDaily https://ift.tt/34RAG7L
from Top Health News -- ScienceDaily https://ift.tt/34RAG7L
Quick look under the skin
Imaging techniques enable a detailed look inside an organism. But interpreting the data is time-consuming and requires a great deal of experience. Artificial neural networks open up new possibilities: They require just seconds to interpret whole-body scans of mice and to segment and depict the organs in colors, instead of in various shades of gray. This facilitates the analysis considerably.
from Top Health News -- ScienceDaily https://ift.tt/3n2XMi5
from Top Health News -- ScienceDaily https://ift.tt/3n2XMi5
Music-induced emotions can be predicted from brain scans
Researchers have discovered what type of neural mechanisms are the basis for emotional responses to music. Altogether 102 research subjects listened to music that evokes emotions while their brain function was scanned with functional magnetic resonance imaging (fMRI).
from Top Health News -- ScienceDaily https://ift.tt/34RO0ZH
from Top Health News -- ScienceDaily https://ift.tt/34RO0ZH
Study suggests link between word choices and extraverts
Psychologists have found a link between extraverts and their word choices.
from Top Health News -- ScienceDaily https://ift.tt/3rvQYga
from Top Health News -- ScienceDaily https://ift.tt/3rvQYga
Chemists develop a new drug discovery strategy for 'undruggable' drug targets
A research team has developed a new drug discovery method targeting membrane proteins on live cells.
from Top Health News -- ScienceDaily https://ift.tt/3aMXRDS
from Top Health News -- ScienceDaily https://ift.tt/3aMXRDS
Switching DNA functions on and off by means of light
Biochemists have developed a new strategy for controlling the biological functions of DNA (deoxyribonucleic acid) by means of light and therefore provide a tool to investigate processes which take place in cells.
from Top Health News -- ScienceDaily https://ift.tt/3nTUI9a
from Top Health News -- ScienceDaily https://ift.tt/3nTUI9a
Do toddlers learning to spoon-feed seek different information from caregivers' hands and faces?
When toddlers begin to use a spoon to eat by themselves, what kind of interactions facilitate this behavior? To find out, an international research collaboration investigated the interactions between toddlers and their caregivers during mealtimes at a daycare center in Japan.
from Top Health News -- ScienceDaily https://ift.tt/3nZJC2k
from Top Health News -- ScienceDaily https://ift.tt/3nZJC2k
Weekly Health Quiz: Vaccines, Grief and the Great Reset
1 How does the normalization of cultured, fake meat fit into the Great Reset agenda?
- It has nothing to do with the Great Reset
- It helps protect the environment, which is a primary goal of the Great Reset
- It's a strategy to take control the part of the food supply that is not already patented
The normalization of fake meat is an attempt to gain control over the part of the food supply that is not already patented. By controlling the food supply in its entirety, the technocrats who promote the Great Reset will control the world's population. Learn more.
- None of the above, because the Great Reset is a fictional conspiracy theory
2 SARS-CoV-2 has been found on:
- Shrimp and salmon
- Beef, chicken and pork
- Air pollution particles
- All of the above
SARS-CoV-2 has been detected on shrimp from Saudi Arabia, fish from India, beef and chicken from Brazil, pork from Germany, salmon from Norway and shrimp from Ecuador. SARS-CoV-2 has also been found on particles of air pollution. Learn more.
3 Imitation meats, such as plant-based and laboratory-grown cell-based meats, are:
- A type of ultraprocessed food, which has been linked to obesity, ill health and early death
The fake meat industry poses tremendous risks to global health as ultraprocessed foods have been robustly linked to obesity, ill health and early death. It also threatens global food security through the patenting of food. Learn more.
- A healthy alternative to conventional meats
- A less expensive and more environmentally friendly alternative to conventional ranching
- Impossible to produce
4 During and after the loss of a loved one, the following increases symptoms of prolonged grief disorder:
- Frequent phone calls from family and friends
- Disruptions to traditional grief rituals, such as saying goodbye, and lack of physical social support
Disruptions to traditional grief rituals, including the ability to say goodbye and viewing and burial of the body, are known to increase symptoms of prolonged grief disorder. Cases also rise when physical social support is absent. Learn more.
- Having the responsibility of preparing a funeral
- Not receiving adequate bereavement leave
5 How many of those who had been in close contact with an asymptomatic individual ended up testing positive, according to data collected from nearly 9.9 million Chinese tested for SARS-CoV-2?
- 100%
- More than half
- Fewer than 25%
- None
Recent data from 9,899,828 Chinese who were tested for SARS-CoV-2 infection found that not a single one of those who had been in close contact with an asymptomatic individual tested positive for COVID-19. Learn more.
6 The high-pitched screaming with arching of the back or inconsolable crying that many parents of vaccine-injured children describe following vaccination are signs of:
- Food allergy
- Fatigue
- Brain inflammation
However, high-pitched screaming with arching of the back or inconsolable crying are signs of brain inflammation. Learn more.
- Pain from the injection site
7 Which of the following, when consumed in excess, can cause you to become insulin resistant?
- Sugar only
- Fructose, specifically
- Unprocessed grains, specifically
- Processed sugar and grains, and omega-6 linoleic acid
Excessive linoleic acid in your diet can produce a negative feedback loop that causes you to become insulin resistant. So, insulin resistance is not restricted to excessive intake of processed sugars and grains. Learn more.
from Articles https://ift.tt/37QYla3
via IFTTT
Time to Defund the Forced Maskers
I've reviewed the science on mask wearing in several articles over the past nine months. So far, there's not been a study showing a significant benefit. On the contrary, evidence is conspicuously piled on the side of the argument that they don't protect the wearer or prevent the spread of infection in community settings.
Despite the lack of scientific basis, universal mask mandates continue to be pushed to ludicrous ends. Case in point: A family was recently booted off a United Airlines flight because the couple's 2-year-old daughter refused to wear a face mask.1
Family Kicked Off Flight Over 2-Year-Old's Mask Refusal
The father, Eliz Orban, spoke to Eyewitness News about the incident in their December 13, 2020, report. United Airlines issued a statement about the event, saying the company has "a multi-layered set of policies, including mandating that everyone onboard 2 and older wears a mask."
United Airlines added that "These procedures are not only backed by guidance from the CDC and our partners at the Cleveland Clinic, but they're also consistent across every major airline." The Orban family were refunded for the flight, and contrary to the couple's original video2 statement, they are not banned from future flights.
This is about as unreasonable as it can get. Not only do universal mask mandates have no scientific backing in general, but insisting that a 2-year-old wear a mask is also nonsensical for the fact that the only way to get what little benefit you can from a mask is by putting it on, wearing and removing properly.
Readers Digest published "11 Mistakes You're Probably Making with Face Masks,"3 reviewing all the ways in which you might nullify the mask's benefit. The idea that a young child would be able to comply with these detailed instructions is beyond unreasonable, seeing how a vast majority of adults cannot even follow them.
One key way by which you negate the benefit of a mask is by touching it. Yet people are constantly fiddling with their masks as they fall down or shift on their face as they talk or move around. A young child is even more likely to contaminate the mask beyond the point of it providing any benefit whatsoever.
Young Children Pose Extremely Low Risk to Others
Importantly though, young children are insignificant disease vectors,4, 5,6,7 meaning they rarely test positive or spread the infection. This makes kicking the family off the plane all the more egregious. In truth, the smartest person in this whole affair is the baby who refused to comply.
Interestingly enough, back in May 2020, United Airlines' COVID-19 policy stressed the need to avoid confrontation. In a statement to CNN for a May 14, 2020, article on airline mask policies, United Airlines said:8
"If for some reason this policy causes a disturbance onboard, we've counseled our flight attendants to use their de-escalation skills, and they do have the flexibility to reseat customers on the aircraft as needed."
Apparently, the flight attendant in this case disregarded such solutions and chose the most traumatic path in dealing with the Orbans instead. Incidentally, while the Orbans are apparently being allowed to fly United Airlines in the future, the company does have a policy that calls for the permanent suspension of noncompliant passengers, according to Forbes.9
Hundreds of Mask Refusers Placed on No-Fly List
The Orbans aren't the first to be kicked off a flight over a mask dispute. According to Delta Airlines CEO Ed Bastian, nearly 700 people have been placed on the company's no-fly list since May 2020 for refusing to wear a face mask.10 The Orbans also aren't' the first to be booted because of an uncompliant child.
September 14, 2020, CNN reported11 that Jodi Degyansky and her 2-year-old son were asked to de-board a Southwestern Airlines flight because her son had his mask pulled under his chin while eating some gummy bears. A flight attendant told Degyansky that families with small children shirk the company's mask policy by eating throughout the entire flight.
Even though Degyansky's son voluntarily put his mask back on, the plane taxied back to the gate and the pair were told to get off. "I feel horrible that my son had to endure that," Degyansky told CNN.12 In August, Southwest Airlines also booted a passenger and her 3-year-old autistic son off a flight after the boy became upset by efforts to force a mask onto his face.13
Defund Forced Maskers
Forcing young children to wear masks for hours on end is ludicrous for all the reasons already mentioned. Even the idea that adults must wear them while flying flies in the face of scientific evidence. My sister recently took a flight during which she noted that first-class passengers were unmasked throughout the entire flight without repercussions. Meanwhile, flight attendants policed everyone else.
If we were really dealing with a lethal virus, wouldn't first-class passengers be as prone to carry and contract it as those with cheaper tickets? And if masks really did work, wouldn't first-class passengers be forced to wear them as well? Enforcement discrepancies alone point to the whole thing being part of a class war and little else.
So, what's the answer? Probably the best strategy would be to "defund" companies that strictly enforce these unscientific rules. In short, don't fly with airlines that boot children off for mask infractions.
What Risk Do Flights Pose?
Do flights pose an infection risk? Probably, yes, for the simple fact that you're in a confined space with many individuals. At least two studies14,15 published in November 2020 have confirmed that infection can and does take place during flights.
Unfortunately, both looked at flights that took place in early March 2020, and neither specify whether passengers were wearing masks or not. Proximity to an infected person appears to be the key finding in these studies, which suggests that spacing out passengers and not filling flights to capacity is the right thing to do to limit transmission.
That said, experts who have looked at available flight data say your risk of catching COVID-19 during a flight is still pretty slim. According to an August 20, 2020, report by CNN:16
"If new scientific claims are borne out, the perceived heightened risk of boarding an airplane could be unfounded. In one case, about 328 passengers and crew members were tested for coronavirus after it was learned that a March 31 flight from the US to Taiwan had been carrying 12 passengers who were symptomatic at the time.
However, all the other passengers tested negative, as did the crew members. And while there have certainly been cases of infected passengers passing the virus on to an airplane's crew or fellow travelers in recent months, the transmission rates are low …
[A] flight from the UK to Vietnam on March 2, in which one passenger seemingly spread the virus to around 14 other passengers, as well as a crew member, is so far believed to be the only known on-board transmission to multiple people.
One explanation for the apparently low risk level is that the air in modern aircraft cabins is replaced with new fresh air every two to three minutes, and most planes are fitted with air filters designed to trap 99.99% of particles …
Arnold Barnett, a professor of statistics at the Massachusetts Institute of Technology's Sloan School of Management, tried to quantify the odds of becoming infected with the virus while on board a short flight in a recent study that looked at the benefits of the empty middle seat policy.
According to his findings, based on short haul flights in the US on aircraft configured with three seats on either side of the aisle … the risk of catching the virus on a full flight is just 1 in 4,300. Those odds fall to 1 in 7,700 if the middle seat is vacant."
Barnett does include mask wearing as one of the factors in his risk calculation. I'm curious how he rated the effectiveness of the masks, seeing how he states that:
"Three things have to go wrong for you to get infected (on a flight). There has to be a COVID-19 patient on board and they have to be contagious. If there is such a person on your flight, assuming they are wearing a mask, it has to fail to prevent the transmission. They also have to be close enough …"
To Pose a Risk, You Need To Be Symptomatic
Studies have repeatedly shown that masks do not significantly reduce transmission of viruses, so it's safe to assume that a mask will in fact fail in this regard. That leaves two key factors: There must be a contagious person onboard, and they must be sufficiently close for transmission to occur.
We now know that asymptomatic individuals — even if they test positive using a PCR test — are highly unlikely to be contagious.17 So, really, a key prevention strategy for COVID-19 seems to be to stay home if you have symptoms. Clearly, forcing a healthy young child to wear a face mask is not going to make the flight any safer.
What Does the Science Say About Masks?
If you're still on the fence about whether masks are a necessity that must be forced on everyone, including young children, I urge you to take the time to actually read through some of the studies that have been published.
As noted by Denis Rancourt, Ph.D., a former full professor of physics and researcher with the Ontario Civil Liberties Association in Canada, all of the well-designed studies that have been published so far have failed to find a statistically significant advantage to wearing a mask versus not wearing one.
Here's a sampling of what you'll find when you start searching for data on face masks as a strategy to prevent viral infection:
|
Surgical masks and N95 masks perform about the same — A 2009 study18 published in JAMA compared the effectiveness of surgical masks and N95 respirators to prevent seasonal influenza in a hospital setting; 24% of the nurses in the surgical mask group still got the flu, as did 23% of those who wore N95 respirators. |
|
Cloth masks perform far worse than medical masks — A study19 published in 2015 found health care workers who wore cloth masks had the highest rates of influenza-like illness and laboratory-confirmed respiratory virus infections, when compared to those wearing medical masks or controls (who used standard practices that included occasional medical mask wearing). Compared to controls and the medical mask group, those wearing cloth masks had a 72% higher rate of lab-confirmed viral infections. According to the authors:
|
|
"No evidence" masks prevent transmission of flu in hospital setting — In September 2018, the Ontario Nurses Association (ONA) won its second of two grievances filed against the Toronto Academic Health Science Network's (TAHSN) "vaccinate or mask" policy. As reported by the ONA:20
|
|
No significant reduction in flu transmission when used in community setting — A policy review paper22 published in Emerging Infectious Diseases in May 2020, which reviewed "the evidence base on the effectiveness of nonpharmaceutical personal protective measures … in non-healthcare settings" concluded, based on 10 randomized controlled trials, that there was "no significant reduction in influenza transmission with the use of face masks …" |
|
Risk reduction may be due to chance — In 2019, a review of interventions for flu epidemics published by the World Health Organization concluded the evidence for face masks was slim, and may be due to chance:23
|
|
"No evidence" that universal masking prevents COVID-19 — A 2020 guidance memo by the World Health Organization pointed out that:24
|
|
Vast majority of COVID-19 patients wore mask — According to the Centers for Disease Control and Prevention25,26,27 71% of COVID-19 patients reported "always" wearing a cloth mask or face covering in the 14 days preceding their illness; 14% reported having worn a mask "often." |
|
Mask or no mask, same difference — A meta-analysis and scientific review28 led by respected researcher Thomas Jefferson, cofounder of the Cochrane Collaboration, posted on the prepublication server medRxiv in April 2020, found that, compared to no mask, mask wearing in the general population or among health care workers did not reduce influenza-like illness cases or influenza. In one study, which looked at quarantined workers, it actually increased the risk of contracting influenza, but lowered the risk of influenza-like illness. They also found there was no difference between surgical masks and N95 respirators. |
|
First COVID-specific mask study fails to show benefit — The first randomized controlled trial29,30 to assess the effectiveness of surgical face masks against SARS-CoV-2 infection specifically, was published November 18, 2020, in the Annals of Internal Medicine.31 It included 3,030 individuals assigned to wear a surgical face mask and 2,994 unmasked controls. Of them, 80.7% completed the study. Based on the adherence scores reported, 46% of participants always wore the mask as recommended, 47% predominantly as recommended and 7% failed to follow recommendations. Among mask wearers, 1.8% (42 participants) ended up testing positive for SARS-CoV-2, compared to 2.1% (53) among controls. When they removed the people who reported not adhering to the recommendations for use, the results remained the same — 1.8% (40 people), which suggests adherence makes no significant difference. Among those who reported wearing their face mask "exactly as instructed," 2% (22 participants) tested positive for SARS-CoV-2 compared to 2.1% (53) of the controls. In conclusion, they found that masks may reduce your risk of SARS-CoV-2 infection by as much as 46%, or it may increase your risk by 23%. |
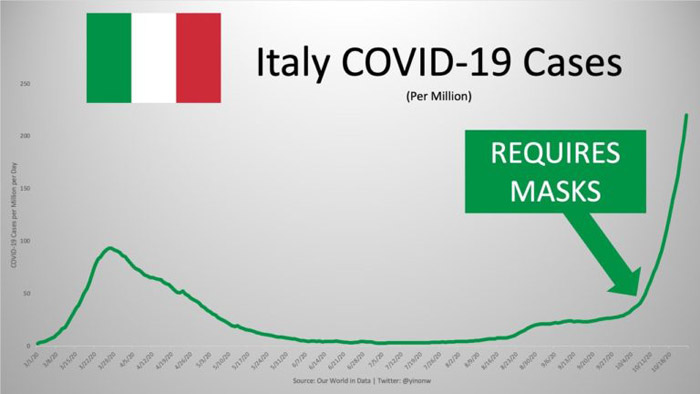
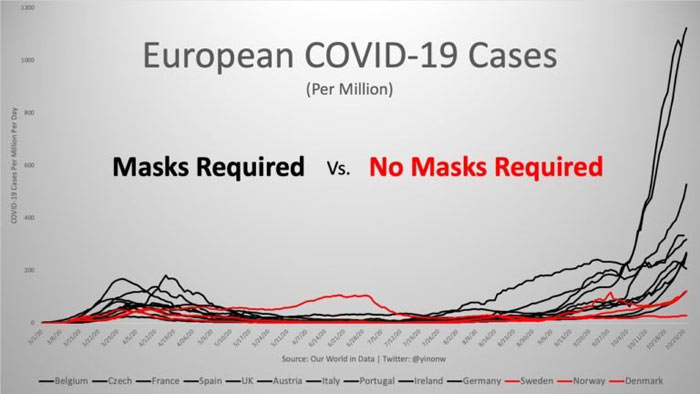
Statistics Show Mask Use Have No Impact on Infection Rates
Another way to shed light on whether masks work or not is to compare infection rates (read: positive test rates) before and after the implementation of universal mask mandates. In his article,32 "These 12 Graphs Show Mask Mandates Do Nothing to Stop COVID," Yinon Weiss does just that.
He points out that "No matter how strictly mask laws are enforced nor the level of mask compliance the population follows, cases all fall and rise around the same time." To see all of the graphs, check out Weiss' article33 or Twitter thread.34 Here are just a select few to bring home the point:



Let's Embrace Reality
Mask wearing, which clearly does little in terms of preventing the rate and risk of infectious spread of SARS-CoV-2, delays the inevitable, which is the acceptance that the disease known as COVID-19 is part of our future, just like the pandemic swine flu H1N1, all the influenza viruses that shift with each season, tuberculosis, Zika and a whole host of other viruses.
We simply cannot prevent any and all COVID-19 deaths any more than we can prevent death from any other cause. All we can do is understand what makes us vulnerable, and take steps to address those underlying weaknesses. In the case of COVID-19, that includes addressing metabolic health, insulin resistance, obesity, and nutritional deficiencies such as vitamin D, magnesium and zinc.
By doing that, you make yourself more resistant to infection and complications thereof. For nine months, the focus has been on masking, social distancing, shutting down businesses and getting a vaccine. Time and again, the goal post has shifted, such that now we're told that even with a vaccine, all of the other measures will still be required well into 2022.
There's a reason why none of it makes sense, and that is because the measures have nothing to do with preventing infection. They're tools used to implement a new economic and social system, as explained in "What You Need to Know About the Great Reset," "Who Pressed the Great Reset Button?" and "Technocracy and the Great Reset."
We need to start presenting a united front against those who seek to destroy society as we know it and steal our assets and resources. One of the first steps toward that end is taking a firm stand against nonsensical and scientifically unjustifiable rules such as universal mask wearing, be it on planes, in stores or outdoors.
While it may not always be possible, consider not frequenting or buying from businesses that kick people out for not wearing a mask. Remember that collectively we have financial clout and, typically, hitting businesses in the pocketbook is the most effective way to demand change.
from Articles https://ift.tt/3mP6G2h
via IFTTT
Sulfur Consumption Reduces Risk of Death
Sulfur is in the top three abundant minerals found in the human body1 and the topic of the interview with Stephanie Seneff, senior research scientist at the Massachusetts Institute of Technology, in the video above. An epidemiological study from West Virginia University found glucosamine sulfate supplements may lower overall mortality as much as regular exercise.2 The underlying mechanism may be related to sulfur.
If you've ever smelled sulfur gas when it comes up from well water, you won't forget the smell of rotten eggs. In fact, the natural gas industry adds mercaptan, a component of sulfur, to natural gas — which has no odor — to make it smell like rotten eggs so you can detect a natural gas leak.3
While stinky in gas form, sulfur is an important mineral in the optimal function of your body. Interestingly, you'll get most of your sulfur from specific amino acids, including methionine, cysteine, cystine, homocysteine, homocysteine and taurine.4 Of these, the two most important are methionine and cysteine. Methionine is an essential amino acid, which means your body can’t synthesize it so it must be supplied through your diet.
Your body can make cysteine from methionine but not from inorganic forms of sulfur. Some individuals are allergic to sulfa drugs and may have concerns about eating sulfur-containing foods. However, since sulfur is an essential element to life, no one is allergic to sulfur. When a sulfonamide molecule from sulfa drugs is metabolized it can bind to a protein that serves as an allergen.5
The sulfonamide molecule in sulfa drugs does have sulfur, but it is embedded in a compound with the unique property of being able to form proteins that cause an allergic reaction in some people. Glucosamine, the subject of the featured publication, is an amino acid that is often combined with sulfate and not known to trigger allergic reactions from the sulfate.6
However, most glucosamine supplements are derived from shellfish and there is some concern of an allergic reaction in people who have an allergy to shellfish.7 There are several forms of glucosamine supplements that are not interchangeable.
They include glucosamine sulfate, glucosamine hydrochloride and n-acetyl glucosamine. Glucosamine sulfate is what is used to help painful arthritis and was the focus of this study.
Study: Glucosamine/Chondroitin Lowers All-Cause Mortality
In an epidemiological study released from West Virginia University, researchers found that individuals using glucosamine supplements had reduced overall mortality to the degree conferred by regular exercise.8 The first author, Dana King, is chair of the department of family medicine at West Virginia University.9
He and his partner, a data analyst, evaluated information from 16,686 adults who had participated in the National Health and Nutrition Examination Survey. The results were from 1999 to 2010 and the data was merged with 2015 mortality figures.
The researchers controlled for a variety of confounding factors, such as age, activity level and smoking status, and found those taking a glucosamine/chondroitin supplement each day for at least a year or longer had a 39% reduced potential of all-cause mortality and a 65% reduction in mortality from cardiovascular-related events.10
King shared that his interest in glucosamine and chondroitin began when he learned many of the cyclists he rode with on weekends used the supplement. King points out that the data are from an epidemiological study and not a clinical trial so it can’t conclusively demonstrate that death is less likely, but goes on to comment:11
“Does this mean that if you get off work at five o’clock one day, you should just skip the gym, take a glucosamine pill and go home instead? That’s not what we suggest. Keep exercising, but the thought that taking a pill would also be beneficial is intriguing.
Once we took everything into account, the impact was pretty significant. In my view, it’s important that people know about this, so they can discuss the findings with their doctor and make an informed choice. Glucosamine is over the counter, so it is readily available.”
The results of this study support previous research published in the BMJ in which researchers engaged 466,039 participants without cardiovascular disease to determine if there was an association between glucosamine use and a reduction in the risk of cardiovascular disease.12
After adjusting for confounding factors, such as age, body mass index, dietary intake, sex and drug use, researchers found there was a “significantly lower risk” of 9% to 22% of all outcome measures.
The outcome measures included cardiovascular disease events, coronary heart disease and stroke in people who used glucosamine supplements daily. The researchers found that their findings supported past studies that had demonstrated an inverse relationship between glucosamine supplementation and cardiovascular disease risk and mortality.
Interestingly, they also found those taking glucosamine and who were current smokers experienced reductions in cardiovascular disease greater than in those who were past smokers or never smokers. They theorized this was because smokers have a higher level of inflammation and glucosamine is associated with a reduction in C-reactive protein, a marker for systemic inflammation.
Sulfur Deficiency May Contribute to Multiple Conditions
An opinion piece that ran in the same publication points out that the sulfate in glucosamine sulfate supplements, which make up “most glucosamine products available on the market,”13 may have been a contributing factor as it satisfies a potential sulfur deficiency.14
One study analyzing how much sulfur is available in the diet concluded “a significant portion of the population that included disproportionately the aged, may not be receiving sufficient sulfur.”15 Scientists are aware that nutrient deficiencies can produce significant health problems.
In one paper in the Journal of the American Heart Association the writers said: “Micronutrients are necessary cofactors for normal cardiac metabolism, and deficiencies have been implicated in the development and progression of HF [heart failure].”16
Seneff and her team proposed the hypothesis that atherosclerosis is the result of a cholesterol sulfate deficiency.17 They proposed that atherosclerosis can be explained by the body using plaque to replenish cholesterol and sulfate to the microvasculature. They argue that insufficient sulfate may increase the risk of high blood pressure and blood clot formation.
Seneff calls sulfur an “unappreciated deficiency” since it is found in several foods and most assume that your diet meets your minimum daily requirements.18 Excellent food sources include eggs, garlic, onions and green leafy vegetables. Nuts, grass fed meat and seafood also contain sulfur.
However, a depletion in the soil creates a deficiency in your fruits and vegetables and may contribute, in part, to sulfur deficiency. She theorizes that a sulfur deficiency is related to rising obesity rates and is connected to glucose metabolism and cardiovascular disease.
In her research, she found people who experience muscle wasting from diseases such as cancer, HIV, sepsis, irritable bowel disease and athletic overtraining may be the result of a deficiency in cysteine and glutathione, two amino acids with sulfur molecules.
MSM Is a Powerful Sulfur Supplement
Sulfur can be found in your muscles, skin and bones. It helps with fat digestion, is needed to make bile acid and required to form collagen.19 The element plays important roles in hundreds of physiological processes. For example, sulfur bonds are needed for proteins to maintain their shape and they determine the biological activity of the protein.
Hair and nails are made of a tough protein called keratin, which is high in sulfur, whereas connective tissue and cartilage have protein with flexible sulfur bonds.20 In addition to proteins, sulfur is also required for the proper structure and biological activity of enzymes.
Methylsulfonylmethane (MSM) is a sulfur donor and contains 34% elemental sulfur by weight.21 Many of the benefits of supplementing with MSM are related to the compound's ability to reduce inflammation, regulate the balance of reactive oxygen species and antioxidant enzymes,22 and modulate your immune response.23 It is widely used in the treatment of pain, especially pain associated with arthritis.
In one clinical trial, researchers found people with osteoarthritis of the knee who took three grams of MSM twice a day for 12 weeks experienced a significant reduction in pain and improvement in physical function, as compared to those who took the placebo.24
In another randomized double-blind placebo-controlled study,25 data showed participants with mild-to-moderate osteoarthritis experienced an analgesic and anti-inflammatory effect when given oral glucosamine and MSM, both individually and in combination.
In this study, the treatment groups received 500 milligrams (mg) of glucosamine and/or 500 mg of MSM three times a day for 12 weeks. According to the authors:
“Combination therapy showed better efficacy in reducing pain and swelling and in improving the functional ability of joints than the individual agents.
All the treatments were well tolerated. The onset of analgesic and anti-inflammatory activity was found to be more rapid with the combination than with glucosamine. It can be concluded that the combination of MSM with glucosamine provides better and more rapid improvement in patients with osteoarthritis."
The Benefits of Bone Broth and Epsom Salts
In addition to food and MSM supplementation, you may also absorb sulfur from homemade bone broth or a relaxing soak in a warm Epsom salt bath. As I've written in the past, bone broth contains other valuable minerals that your body can easily absorb in use, including magnesium, phosphorus, calcium, silicon, sulfur chondroitin and glucosamine.26
Bone broth also helps attract and hold liquids in the digestive system and supports proper digestion. In one study, researchers found that chicken soup has medicinal qualities and significantly mitigated inflammation and infection.27,28 The amino acids in bone broth helps to fight inflammation and courtesy of chondroitin sulfate and glucosamine, it helps to reduce joint pain and inflammation.29
Bone broth is made from animal bones. It's important to use homemade bone broth since the store-bought variety is produced by adding chemical-laden bouillon cubes, whereas traditional soups are made by cooking bones and meat for several hours. In its simplest form, it's made by using bones, vinegar and spices, and simmering in a pot or slow cooker for as long as 24 to 72 hours.
Bone broth made over longer periods of time increases the release of gelatin, minerals and other nutrients from the bones, which are key to many of the benefits and restorative properties.
Epsom salt baths are a simple way of absorbing both magnesium and sulfate. Epsom salt is magnesium sulfate, which is easily absorbed through your skin. It is also a preferable way of absorbing magnesium and sulfate since it's readily available to your body without having to be converted as it is when taken orally.
As a general recommendation, use 1 to 2 cups of Epsom salt in a tub of water. The warmer the water, the more the salt will dissolve and the more your body will be able to absorb it.
Some people may experience a negative reaction, such as irritability or hyperactivity. In this case, decrease the amount you use and incrementally raise it based on your tolerance. Alternatively, make a foot bath of one part Epsom salt to two parts water and soak your feet for about 30 minutes.
from Articles https://ift.tt/3aO67nk
via IFTTT
MKRdezign
Powered by Blogger.