If there is an injury to the central nervous system such as after a stroke, the brain needs to compensate for this by reorganising itself. To do this, a dense network of molecules between the nerve cells -- known as the extracellular matrix -- must loosen. This is the job of a wide variety of enzymes that ultimately regulate how plastic or how stable the brain is. Researchers studied what happens when certain enzymes are blocked in mice. Depending on whether the brain is healthy or diseased, the inhibition had opposite effects.
from Top Health News -- ScienceDaily https://ift.tt/3GGRkqV
As emissions fell over a decade, the number of deaths attributable to air pollution dropped by thousands, yielding billions of dollars in societal benefits.
from Top Health News -- ScienceDaily https://ift.tt/3IOn4fP
Researchers have solved a major mystery in cancer research: How cancer cells remain dormant for years after they leave a tumor and travel to other parts of the body, before awakening to create metastatic cancer.
from Top Health News -- ScienceDaily https://ift.tt/3yobFyt
In Bannons War Room interview above, Dr. Robert Malone, inventor of the mRNA and DNA vaccine core platform technology,1 reviews what we know so far about the so-called Omicron variant of SARS-CoV-2.
As noted by Malone, the latest media hype actually began with reports of Africa having far lower case rates than the rest of the world, despite its comparatively low COVID jab rate. That was followed by reports in the local press that South Africa was asking Pfizer to halt its shipments of the shots, as they still had plenty and most adults were refusing to take it.
The very next day, “we suddenly had this huge kerfuffle about this new virus strain, and the press was announcing it was coming out of South Africa,” Malone says. The U.K. almost immediately responded by shutting its borders to most of South Africa.
According to media reports, the Omicron variant was discovered in Botswana, in four fully “vaccinated” individuals. Physicians in South Africa responded saying that while the variant has been detected, they are not seeing significant illness from it. All cases so far have been mild and none has required hospitalization.
Coordinated Fear Porn Campaign
In rapid succession, news articles were published proposing the virus evolved in an AIDS patient and appears to spread far easier than previous variants. Calls for concern and the need for new restrictions flooded the airways. As noted by Malone, the press was talking about “everything except for the obvious, which is that this is a ‘vaccine’-escaped mutant.”
Indeed, the variant appears highly resistant to the COVID shots, which is a sign of it having mutated within one or more COVID-jabbed individuals, not in someone with no antibodies at all to attack it.
Remember, viruses mutate primarily in response to insufficient immune responses. Yet among the first recommendations from the mental giants in charge of COVID responses was to push COVID booster shots, which is as irrational as it is unscientific.
“The boosters are a perfect way to bias our immune system so we’re LESS able to respond to this new variant,” Malone explains. “This is [like] jabbing everybody with a flu vaccine from three seasons ago and expecting it to have effects against the current [flu strains].”
Is Omicron Another Lab Creation?
As for the nature and origin of Omicron, Malone says:
“It has the hallmark of a viral agent under tight genetic selection for evolution to escape the ‘vaccine’ responses against the receptor bonding domain. The question that is outstanding right now is — because this is so different from the other strains that are being tracked; it’s in its own separate little evolutionary branch — how did this happen? Why did this suddenly pop up with all these new mutations?”
The mainstream press is pushing the narrative that Omicron’s mutations are due to the low COVID jab rate in South Africa, possibly in combination with it mutating within someone with AIDS. The solution, we’re told, is to blanket Africa with COVID shots, even though the continent has enjoyed a phenomenally low case rate and mortality rate without the jabs. So, clearly, this narrative is trying to achieve an end that simply isn’t warranted by the real-world data.
Aside from shaming South Africa into getting more COVID shots, another potential reason for this narrative is that they want to hide that it’s another lab created virus. As noted by Malone, we have “the looming specter of this being further engineered in some way.”
In all, Omicron is said to have some 50 mutations from the original Alpha strain, many of which specifically allow it to circumvent COVID shot-induced antibody defenses.
While Malone admits he is not closely tracking the mutations of the virus, and is not qualified to speculate on its evolution, he points out there is a subset of experts who believe it may have undergone lab modification because, genetically, it “doesn’t look like it’s part of the prior evolutionary process that we’re seeing with many other strains.”
Until and unless we end up with conclusive proof of its origin, we need to keep all options open, Malone says, and that includes the possibility of Omicron being cooked up in a lab from a previous strain.
Omicron Cases Double in Less Than Five Days
So far, we know as little about Omicron as we did the original SARS-CoV-2 virus when it first emerged. What we do know is that it appears highly infectious, doubling in a median time of 4.8 days, and has significant “vaccine” evasion capabilities.2
According to the Economist,3 which cites data from South Africa’s National Institute for Communicable Diseases, Omicron “appears to have rapidly outcompeted Delta” in South Africa, as of the first week of December 2021 accounting for nearly all positive cases.
One particularly odd feature of Omicron is that the closest genetic sequences date back to mid-2020. It doesn’t seem to belong to any of the evolutionary branches that have emerged since. As noted by professor Trevor Bedford, a computational virologist interviewed by NPR, “This is very rare to see.”4
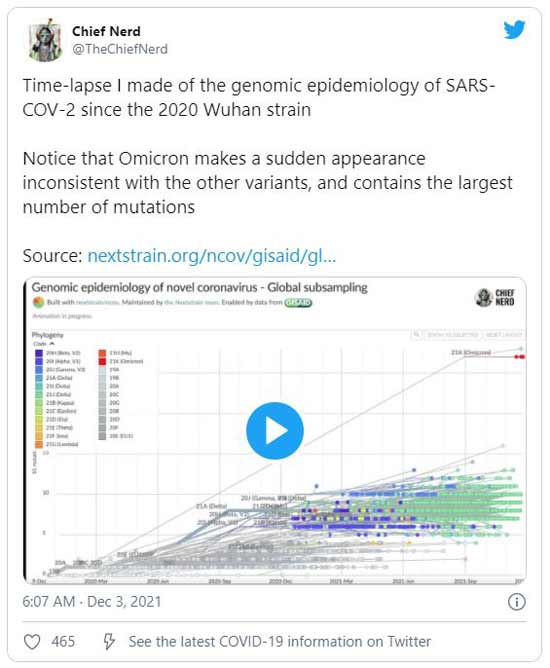
In a Twitter post, a user named Chief Nerd, shows a time-lapse graphic5 he created that illustrates the genomic epidemiology of SARS-CoV-2 from the original strain until now, using data from nextstrain.org.6
It’s a great illustration of just how odd an unnatural Omicron’s emergence really is. As the time-lapse gets toward the end of 2021, suddenly there’s Omicron, emerging like a straight line from a mid-2020 strain, having no semblance to any of the other strains.
There’s no precedent for this oddity occurring in nature. There is, however, precedent for this in lab-leaked pandemics, such as the 1977 Russian influenza, caused by an H1N1 flu strain that strongly resembled a strain in circulation between 1946 and 1957. There have been persistent rumors that the Russian flu might have been the result of a live-vaccine trial escape.7
Omicron, also known by the designation B.1.1.529., has a ratio of nonsynonymous to synonymous mutations of 25 to 1. According to molecular biologist and cancer geneticist Philip Buckhaults, Ph.D.,8 Omicron has 25 nonsynonymous and only one synonymous spike mutation compared to its most recent common ancestor, AV.1. Were it a natural occurrence, that ratio ought to be somewhere between 25 to 50 and 25 to 100.
Three Hypotheses of Omicron’s Origin
Researchers have tried to explain this phenomenon in a variety of ways. Bedford has suggested the mid-2020 strain might have infected and evolved within some unknown animal population before spilling back into the human population.
It’s an unlikely scenario though, Bedford says, because there ought then to be signs of the animal genetic material in the genome, and we’re not seeing that. Instead, there’s human RNA insertions, which suggests a human host.
Another hypothesis is so-called “cryptic spread” in an unmonitored region. In other words, the mid-2020 strain may have circulated in an area where testing and monitoring of cases were low or absent, allowing it to evolve under the radar, until finally becoming transmissible enough to spread into more monitored regions.
Alas, Bedford finds fault with this explanation as well, “Because it would seem that as [this strain of the virus] was on its path to becoming Omicron and becoming a quite transmissible virus, [the earlier versions] would have started to spread more widely before just now.”9
A third hypothesis involves the incubation in an immunocompromised patient, such as an AIDS patient. If the patient’s immune system was just robust enough to prevent death, but not complete clearance, the virus may have lingered for many months, slowly mutating over time.
The crux here is that the virus ought to have spread from that person earlier. Why did it take well over a year for it to finally be transmitted? Intermediate variants should have emerged, but didn’t. It just suddenly emerged with dozens of mutations already baked in that have no precedent.
Bedford told NPR,10 "That's a good question and a legitimate one. I don't have an obvious answer besides chance." Despite the lack of plausible answers, Bedford believes this scenario may be the most plausible.
Two Elephants in the Room — The Missing Hypotheses
Of course, getting back to Malone’s observation, what’s missing from this list of hypotheses is the most obvious one, which is that the virus mutated in response to the pressure of widespread COVID injections. Also missing is the hypothesis that Omicron was genetically manipulated from a mid-2020 strain, and in one way or another entered into circulation.
Irrationally, Bedford and others are now stressing the importance on ramping up HIV treatment to prevent mutations from occurring in untreated individuals with low immune function, rather than taking a long hard look at how the mass “vaccination” campaign is driving the evolution of this virus and putting COVID jabbed individuals at ever-increasing risk of serious infection.
At present, one of the most plausible theories appears to be that scientists enabled an early SARS-CoV-2 variant to build antibody resistance, possibly by passaging them through human or humanized cell lines in the presence of convalescent plasma.
The Lab in South Africa Experimented on SARS-CoV-2
If Omicron is another lab creation, what lab might be responsible for its creation? A number of internet sleuths have pointed fingers at the biosafety level 3 (BSL3) lab in Durban, South Africa, where research on SARS-CoV-2 was taking place.
A paper titled “Escape of SARS-CoV-2 50IY.V2 from Neutralization by Convalescent Plasma”11 was published in the journal Nature at the end of March 2021. This appears to be just the kind of research that might train the virus to evade COVID antibodies.
The research, funded by the Bill & Melinda Gates Foundation, was conducted by a conglomerate of researchers, most from South Africa, but also one American and several with research credentials at both South African and German, British or American research facilities. Affiliates listed include several research facilities in South Africa, as well as research institutes in Israel, the U.K., U.S., Germany and Brazil.
In a series of December 3, 2021, Twitter posts,12 Yuri Deigin, a drug developer and biotech entrepreneur, points out that the initial emergence of Omicron was in Durban, where the BSL3 lab happens to be located, and where that study was done.
As yet, the Omicron lab leak theory is loosely held together, but if recent history is any indication, we’re bound to start seeing more extensive discussions and reviews of the evidence as we go along.
As noted in an October 10, 2021, New York Post editorial,13 the lab leak theory, referring to the original SARS-CoV-2 virus, “is now almost certainly proved” — and according to David Martin, Ph.D., proved beyond all doubt based on the patent trail, dating back two decades14 — but it took well over a year and a half to get to this point.
While the Omicron origin question is likely to grow, our fear of this variant doesn’t have to. So far, all indications are that Omicron is among the mildest of the variants — highly infectious with rapid spread, but very mild in terms of symptoms.
This article was previously published October 8, 2020, and has been updated with new information.
According to the World Health Organization, ischemic heart disease and stroke were the top two causes of death across the world in 2016.1 Although there have been dramatic declines in cardiovascular diseases (CVDs), ailments in this category continue to remain major causes of loss of health and life.2
In the U.S., the CDC's Division for Heart Disease and Stroke Prevention reports that 1 in every 3 deaths is from heart disease and $1 of every $6 is spent on CVD.3
While the statistics are disturbing, cardiovascular disease can also lead to nonlethal stroke, heart attack, disability, serious illness and a lower quality of life. These conditions can trigger fatigue, depression and related problems.
The American Heart Association tracks seven key health factors and behaviors they believe increase your risk for heart disease and stroke.4 They call these "Life's Simple 7," which they measure to track progress toward their goal of improving the cardiovascular health of people in the U.S.
While each of Life's Simple 7 behaviors and risk factors are important to overall health, they do not address problems with sleep as contributing factors.
Pandemic Interfering With Sleep Hours and Quality
In an interview with KYW radio, Dr. Zeeshan Khan, pulmonologist from the Deborah Heart and Lung Center, talked about sleep disorders and the relationship they have with CVD, especially in the midst of the current pandemic.5 He told the reporter that the International Classification of Sleep Disorders identifies at least 60 diagnoses in seven categories.6
The two most common are insomnia and obstructive sleep apnea. With sustained poor sleep, a person may experience altered judgment, mood swings and impaired cognition. Khan also listed problems with the cardiovascular system and immunity in people who chronically get less than seven hours of sleep each night.
He warned that lack of sleep can lead to problems with a person's general health. He recommends that on average, people should get seven hours of sleep each night, but he also shared that in America, about 35% of the people get less than that. "We are kind of a sleep-deprived nation," he said.
Symptoms of disrupted sleep or insomnia can vary depending on the person. Although you may take a 30-minute power nap in the early afternoon, it doesn't get rid of sleep debt. It may help you feel better in the immediate moment, but it doesn't impact the effect of sleep debt on your overall health.
Lack of Quality Sleep Is Associated With Cardiac Morbidity
When asked about how long it should take to fall asleep, Khan said the average amount of time is 15 to 20 minutes. However, the time it takes to fall asleep is extended when people take their smartphone or computer to bed with them. Using these devices can disrupt sleep in several ways, including by engaging your mind at a time when it should be slowing down.
Khan advises people to first use nonpharmacological treatments to help them sleep, such as cognitive behavioral therapy, mindfulness, a consistent sleep routine and meditation. He also recommends steering clear of medications as they can be addictive and they only treat the symptom of sleep disruption, not the reason behind it.
Additionally, he recommends steering clear of having a nightcap to help you relax and fall asleep. This is because drinking alcohol before bed may help you fall asleep faster, but in the long term it can have a negative effect on your sleep patterns. He stresses the importance of using a routine to go to sleep to cue your biological clock.
He went on to discuss the problems with sleep apnea, which often overlap with snoring. During snoring the upper airway narrows, which causes vibrations in the membranes. Although most people with sleep apnea snore, not all people who snore have sleep apnea.
When people with diabetes, heart disease or other problems also snore, they should be evaluated for sleep apnea, especially if they start having problems during the day. Sleep apnea lowers the amount of oxygen delivered to the brain, heart and other organs during sleep. According to Khan:7
"Almost every cardiac morbidity you can think of has been linked to sleep apnea. Heart disease, heart failure, arrhythmias, strokes … inflammatory issues like diabetes, worsening obesity — the list can go on and on."
Sleep Disorders Associated With Using Technology at Night
In a recent study in Sleep Standards, researchers evaluated the results from a survey of 1,062 people across the U.S.8 The objective was to gain an understanding of how technology may have a relationship with sleep disorders.
One key finding was that 71.8% of the respondents who reported a disruption in sleep pattern also used technology just before bed. The researchers separated the participants into five age groups, which represented the total number in the survey. They were:
Generation Z (under 25) — 22.3%
Millennials (26 to 40) — 44.8%
Generation X (41 to 55) — 23.8%
Baby Boomers (56 to 76) — 8.9%
Silent Generation (older than 76) — 0.2%
They also found that those under age 25 were the most likely to have sleep disorders. People who had a sleep disorder averaged five hours of sleep per night and spent up to 20 hours in front of a bright screen each day.9 The participants also reported that they used their technology devices within 30 minutes of bedtime: 70.2% watched television; 59.4% checked social media; 31.8% checked email; and 32.9% played video games.10
Of all the participants, 57.8% said they used cell phones, which was higher than television use at 18.5% or computer use at 14.2%. The highest percentage of participants in the survey had insomnia at 64.3%.
Although sleep apnea was the second most common disorder, it ran a far second at 14%. Other disorders reported in the survey included sleep paralysis, parasomnias, restless leg syndrome and narcolepsy. Although many experts such as Khan recommend steering clear of pharmaceutical remedies to treat insomnia, 51.2% of those surveyed reported using sleeping pills and 47.5% had tried other medications.
Sleep Deprivation Associated With More Health Conditions
Fragmented or disturbed sleep happens when you fall asleep easily but awaken during the night. This may happen frequently, and you go back to sleep easily, or you awaken and have a hard time going back to sleep. This type of sleep pattern can trigger chronic inflammation that contributes to mental health issues and neurological disorders.11
Lack of sleep also affects your immune system by reducing the number of protective cytokines available.12 In addition, it is associated with atherosclerosis, which is the buildup of plaque in the arteries. This may be called "clogged" or "hardened" arteries and can lead to lethal heart disease.
The exact mechanism of poor sleep in inducing atherosclerosis may have been clarified in a study published by UC Berkeley sleep scientists, who found that an increase in neutrophil and monocyte levels during fragmented sleep had an impact on the pathology of atherosclerosis. They wrote:13
"… these findings affirm a pathway in which the quality of human sleep, specifically the degree of fragmentation, raises inflammatory-related white blood cells, thereby conferring increased risk for atherosclerosis. This was true of sleep fragmentation assessed across a week or across a single night, which predicted increasingly higher CAC [Coronary Artery Calcification] score through a mediating association with increased neutrophils."
Sleep deprivation is also linked to the development of Alzheimer's disease and other neurodegenerative conditions. A recent animal study from Marche Polytechnic University in Italy revealed that astrocytes in the brain will start to break down healthy nerve synapses when you are chronically sleep deprived.14 They wrote that the results suggested:
"… that like many other stressors, extended sleep disruption may lead to a state of sustained microglia activation, perhaps increasing the brain's susceptibility to other forms of damage."
Average Number of Sleep Hours Dropping
For several years Mattress Firm has commissioned a survey on sleep habits and the number of hours people are sleeping each night. The 2019 results show Americans are sleeping less and less. They asked 3,000 adults about their sleep habits, how satisfied they were with their sleep and about the frequency of sleeping and naps. They compared those results to those from 2018.15
What they found was a sad commentary on the speed at which modern society has chosen to live. It seems that getting at least six hours has become more challenging with each passing year. In 2018, results from the survey showed the average person was sleeping six hours and 17 minutes each night, but by 2019 that had dropped to 5.5 hours.16
Experts currently recommend adults from 18 to 65 years sleep consistently from seven to nine hours each night.17 In other words, most people are sleeping at least 1.5 hours less each night than the minimum that experts think is important for optimal health.
While the number of hours you sleep is important, so is the quality. So, it's even more disheartening to read that 25% of the respondents reported they also "consistently slept poorly in 2019."18
Since the amount of quality sleep at night was on the decline, it makes sense that respondents reported they took more naps in 2019 than 2018. But, while more were taken, survey findings indicate there were many planned naps that didn't get taken.
The survey defined a "great night's sleep" as "quickly falling asleep and staying that way until morning." There were about 120 nights fitting that criteria. Americans are so desperate for a good night of sleep they said they were willing to "pay $316.61 for just one night of perfect sleep." This was $26.16 more than in 2018.
Interestingly, the people who reported the best sleep were those who slept on their back or slept with a pet in their bed. While side sleeping was the more common position reported in the survey, these were the same respondents who had the most difficult time getting to sleep.
EMF Pollution Associated With Sleep Hours and Quality
As I've written before, your sleep quality may be impacted by several factors, including your sleep pattern, the number of hours you spend sleeping and by the light and electromagnetic pollution in your area. If you've ever gone camping, you may have noticed a change in your sleep quality. Chances are you had a deeper sleep and awakened more rested.
Two factors that influence sleeping better outdoors are the drastic reduction in artificial lights and the reduction in electromagnetic fields (EMF). Your circadian clock is affected by your melatonin levels, which in turn are affected by exposure to light at night. You might enjoy the same restful sleep if you install blackout blinds, use a sleep mask and get rid of any light-emitting source in your bedroom.
Electromagnetic fields also may impair sleep quality19 and produce oxidative damage during sleep.20 Consider shutting off all your electronic devices and your Wi-Fi modem and router at night to reduce your exposure and improve your sleep quality. For more tips on improving the number of hours you sleep and the quality of your sleep, see "Top 33 Tips to Optimize Your Sleep Routine."21
When a woman is pregnant, she is truly eating for two. Every food, medication, supplement and drug affects her growing baby. Her body also produces different levels of hormones to support the pregnancy. Each month, a woman's body cycles through a variety of hormones that regulate the buildup of blood in the uterus to support a pregnancy, the maturation of an egg and the withdrawal of hormones that lead to menstruation.1
Progesterone is one of those hormones and the one that is often called the “pregnancy hormone”2 because of the important role it plays, from implantation of the embryo to delivery of the baby. After the egg is released from the ovary, the corpus luteum produces progesterone to maintain the early stages of pregnancy.3
The corpus luteum is a group of cells that form just after the egg leaves the ovary. The progesterone makes the uterus a healthy environment for a fertilized egg to implant and begin to grow.4 As the fertilized embryo implants, progesterone stimulates the further growth of blood vessels and triggers the endometrium to secrete nutrients to support growth.
During these early weeks, progesterone is essential to establish the placenta. As the placenta is established, it takes over producing progesterone at around Week 12. During the remaining two trimesters, progesterone levels continue to rise and play a role in strengthening the pelvic wall muscles, preventing lactation and growing of the mother's breast tissue.
Scientists have not identified serious medical consequences of producing too much progesterone,5 yet supplementing with progesterone when you aren't pregnant has been associated with a small risk of developing breast cancer.6 However, without enough progesterone women can experience irregular and heavy menstrual periods and a drop in progesterone levels can lead to miscarriage.
Progesterone May Help Prevent Early Miscarriage
The National Institute for Health and Care Excellence (NICE) has recommended that women who experience bleeding early in pregnancy and have had at least one miscarriage be offered progesterone supplementation to reduce the risk of losing another pregnancy.7 The guidance was based on research evidence that showed women with more miscarriages had better results with progesterone supplementation.8
According to the article in the BBC,9 1 in 5 pregnant women experience spotting in the first 12 weeks of pregnancy. This is light bleeding that occurs intermittently. If bleeding occurs alongside the pregnancy, this is called a threatened miscarriage. Today, most women with bleeding are sent home and asked to wait to see what happens.
However, new guidance from NICE recommends using a progesterone pessary in the vagina twice a day to deliver progesterone supplementation that supports the pregnancy.10 One trial carried out at Tommy's National Center for Miscarriage Research showed those who had bleeding and no previous miscarriages didn't experience benefits from progesterone supplementation.
Past research has evaluated the use of progesterone to support pregnancy. One study11 published in 2005 looked at randomized controlled trials of women who received progesterone supplementation before 34 weeks gestation. The data indicated it reduced the incidence of preterm birth in high-risk women.
A second paper12 published in 2013 found the results of 17 trials showed no evidence to support the use of progestagens for the treatment of threatened miscarriage. A third animal study13 published in 2020, analyzed the use of progesterone during early pregnancy on fetal development.
They found administration could alter the pituitary and testicular function in male children. The results suggested progesterone had a sex-specific effect in early pregnancy and should be used only “when there's clear evidence of efficacy and for as limited time as necessary.”14
Progesterone May Prevent 8,450 Miscarriages Each Year
The NICE guidance was based on studies published in 2020, which found progesterone given to women with bleeding in early pregnancy could prevent 8,450 miscarriages each year. Both studies were published January 30, 2020. The study published in the American Journal of Obstetrics and Gynecology15 examined the results of two major clinical trials that were led by Tommy's National Center for Miscarriage Research and the University of Birmingham.
The clinical trials were the Progesterone in Recurrent Miscarriage trial (PROMISE)16 and Progesterone in Spontaneous Miscarriage trial (PRISM).17,18 The PROMISE trial studied 836 women at 45 hospitals in the Netherlands and U.K.19 The data revealed that those with recurrent miscarriages had a 2.5% higher live birth rate when supplemented with progesterone.20
In the PRISM trial,21 4,153 women from 48 hospitals in the U.K. were given progesterone with early pregnancy bleeding. The data revealed there was a 5% increase in live birth compared to those given a placebo. In women with three or more miscarriages, the data showed a 15% increase in the number of babies born to those given progesterone.22
The second study on which the NICE guidance was based was published in BJOG: An International Journal of Obstetrics & Gynaecology.23 This paper looked at the economics of the PRISM trial and concluded the average cost of treatment was £204 ($272.19) per pregnancy. They concluded that:24
“The results suggest that progesterone is associated with a small positive impact and a small additional cost. Given available evidence, progesterone is likely to be a cost-effective intervention, particularly for women with previous miscarriage(s).”
Women who are not pregnant may have symptoms of low progesterone that include irregular menstrual cycles, vaginal dryness, mood changes, headaches or migraines. Progesterone helps to complement estrogen during a normal menstrual cycle.25 Without the effect of progesterone, estrogen may increase the risk of weight gain, breast tenderness, fibroids and gallbladder problems.
Different Types of Administration of Progesterone
Not all forms and types of progesterone are created equally. Doctors prescribe progesterone to regulate the menstrual cycle, treat hyperplastic precursor lesions in the endometrium and as a contraceptive.26 Synthetic progesterone27 may be associated with birth defects, so it is important to be sure you are using a natural source and always consult with your health care provider when using progesterone, whether you are pregnant or not.
Progesterone can come as a vaginal gel, suppository, insert, oral capsule or injection.28 Vaginal gels are used once a day and are the only FDA-approved product for assisted reproduction, such as in vitro fertilization. Thus far there have been over 40 million doses prescribed in the past decade.
Vaginal suppositories are wax-based and inserted two to three times a day. However, leaking can be messy and although they are widely used, they are not FDA-approved. Vaginal inserts are approved for supplementation but not progesterone replacement.
While they are not formulated or FDA-approved for vaginal use, progesterone oral capsules have been used vaginally, up to three times a day, as they have fewer side effects when used vaginally, than when taken orally.
Finally, progesterone can be given as an oil-based injection. It's the oldest method of delivery and is injected into the buttocks once daily. Because it's oil-based, the injections can be painful and skin reactions are common.
Women who use progesterone supplementation in early pregnancy may experience some side effects. These side effects should be reported to their health care professional as soon as possible.29,30,31
Abnormal vaginal bleeding
Breast changes or discharge
Vision changes
Allergic reactions
Chest pain
Problems talking and walking
Confusion
Severe headaches
Dark urine
Flu-like symptoms
Sudden numbness or weakness
Pain, swelling, warmth in the leg
Shortness of breath
Nausea and vomiting
Light-colored stools
Loss of appetite
Right upper belly pain
Unusual fatigue
Yellowing of the eyes or skin
Stomach cramps
Bloating
Back pain
Depressed mood
Mood swings
Increased appetite
Fluid retention
Added Challenges if You Are Pregnant During the Pandemic
Women who are pregnant during the pandemic have a few added challenges to stay healthy and protect the health of their child. Pregnancy places a higher demand on pulmonary functions. Thus, women with underlying medical conditions such as heart disease, diabetes, high blood pressure or lung problems may have a higher risk of infection and severe disease.
It is important to communicate any changes with your doctor, such as decreased fetal movement, or if you believe you're having signs of preterm labor. Researchers believe up to 80% of those with COVID-19 will have mild symptoms or be asymptomatic.32 This is similar to studies done with flu in England, which found the majority of those were asymptomatic.33
This means you need to take care even with individuals who appear to be healthy. A vital step in prevention is excellent handwashing for at least 20 seconds and avoiding touching your face.
You also need to be aware that taking supplements or medications during pregnancy can have affects on your growing baby that are not always well understood or documented. Even commonly accepted over-the-counter medications and supplements may have long-term consequences.
For example, there is evidence to suggest that acetaminophen, commonly sold as Tylenol, may double the risk of autism34 and increase the risk of attention deficit disorders in children.35
It is also crucial to maintain healthy levels of vitamin D during your pregnancy. In one Cochrane systematic review,36 the authors found evidence that vitamin D could reduce the risk of preeclampsia, low birth weight and preterm birth. It also plays a functional role in reducing the risk of upper respiratory infections,37 which includes flu and COVID-19.
Vitamin C plays a role in the treatment of COVID-19, but large doses should not be used preventively. To protect your health, seek out foods that are high in vitamin C,38 such as bell peppers, kiwi fruit, strawberries, broccoli, tomatoes and snow peas.