Rockefeller Foundation's Plan to Track Americans
Bill Gates — who illegally invests in the same industries he gives charitable donations to, and who promotes a global public health agenda that benefits the companies he’s invested in — has gone on record saying life will not go back to normal until we have the ability to vaccinate the entire global population against COVID-19.1
To that end, he is pushing for disease surveillance and a vaccine tracking system2 that might involve embedding vaccination records on our bodies. One example of how this might be done is using an invisible ink quantum dot tattoo, described in a December 18, 2019, Science Translational Medicine paper.3,4
According to statements made by Gates, societal and financial normalcy may never return to those who refuse vaccination, as the digital vaccination certificate Gates is pushing for might ultimately be required to go about your day-to-day life and business. Without this “digital immunity proof,” you may not even be allowed to travel locally or visit certain public buildings.
Gates has a history of “predicting” global pandemics with vast numbers of deaths,5 and with his call for a tracking system to keep tabs on infected/noninfected and vaccinated/unvaccinated individuals, he’s ensuring an unimaginably profitable future for the vaccine makers he supports and makes money from via his Foundation investments.
Along with Gates, The Rockefeller Foundation is also coordinating efforts in the direction of social control through the implementation of draconian COVID-19 tracking and tracing measures that are clearly meant to become permanent.
National COVID-19 Testing Action Plan
April 21, 2020, The Rockefeller Foundation released a white paper6 titled, “National COVID-19 Testing Action Plan — Strategic Steps to Reopen Our Workplaces and Our Communities.” In the foreword, Rockefeller Foundation president Dr. Rajiv J. Shah writes:
“In the face of an ineffective nationally-coordinated response, insufficient data, and inadequate amounts of protective gear and testing, we need an exit plan. Testing is our way out of this crisis.
Instead of ricocheting between an unsustainable shutdown and a dangerous, uncertain return to normalcy, the United States must mount a sustainable strategy with better tests and contact tracing, and stay the course for as long as it takes to develop a vaccine or cure.
Any plan to do so must win the faith of private and public sector leaders across the country, and of individual Americans that they and their loved ones will be safer when we begin to return to daily life.
The Rockefeller Foundation exists to meet moments like this. In the past two weeks we have brought together experts and leaders from science, industry, academia, public policy, and government — across sectors and political ideologies — to create a clear, pragmatic, data-driven, actionable plan to beat back Covid-19 and get Americans back to work more safely.”
The plan calls for testing and tracing 1 million Americans per week to start, incrementally ramping it up to 3 million and then 30 million per week (the “1-3-30 plan”) over the next six months until the entire population has been covered.
Test results would then be collected on a digital platform capable of tracking all tested individuals so that contact-tracing can be performed when someone tests positive. According to the “National COVID-19 Testing Action Plan”:
“Policy makers and the public must find the balance between privacy concerns and infection control to allow the infection status of most Americans to be accessed and validated in a few required settings and many voluntary ones.”
To this end, they suggest using incentives “to nudge the voluntary use” of tracking and contact tracing apps rather than making them mandatory. They also call for the use of “innovative digital technologies” aimed at improving “workforce monitoring and early detection of recurrent outbreaks.”
“When integrated into national and state surveillance systems, such innovations may enable the same level of outbreak detection with fewer tests.
Promising techniques include anonymous digital tracking of workforces or population-based resting heart-rate and smart thermometer trends; continually updated epidemiological data modeling; and artificial intelligence projections based on clinical and imaging data,” the document states.7
Modern ‘Wartime’ Effort That Will Cost Billions
According to the “National COVID-19 Testing Action Plan”:8
“Monitoring the pandemic and adjusting social distancing measures will require launching the largest public health testing program in American history ... The effort will ultimately grow to billions of dollars per month ... But with widespread business closures costing the country $350 billion to $400 billion each month, the expense will be worth it.
This testing infrastructure is intended to tide the country over until a vaccine or therapy is widely available.
Coordination of such a massive program should be treated as a wartime effort, with a public/private bipartisan Pandemic Testing Board established to assist and serve as a bridge between local, state, and federal officials with the logistical, investment and political challenges this operation will inevitably face.”
Don’t Be Naïve About Infectious Tracking Plan
Call me jaded, but this sounds like a plan to surveil Americans so that they can easily be tracked down for mandatory vaccination once a COVID-19 vaccine becomes available. It also creates the necessary infrastructure for vaccination tracking across the board, for all vaccines.
While they give lip-service to privacy and anonymization of data, privacy promises have been repeatedly broken in the past. Besides, the document clearly states that:9
“Some privacy concerns must be set aside for an infectious agent as virulent as Covid-19, allowing the infection status of most Americans to be accessed and validated in a few required settings and many voluntary ones.
The loss of privacy engendered by such a system would come at too high of a price if the arrival of a vaccine early next year was a certainty. But vaccine development and manufacture could take years, and when it comes certain populations may be excluded from receiving it for health reasons.
In the meantime, infection status must be known for people to participate in many societal functions. Legislation protecting people from being fired over infection status must be passed.
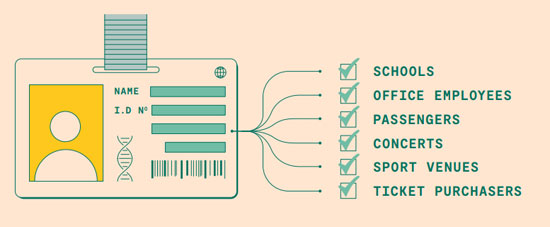
Those screened must be given a unique patient identification number that would link to information about a patient’s viral, antibody and eventually vaccine status under a system that could easily handshake with other systems to speed the return of normal societal functions.
Schools could link this to attendance lists, large office buildings to employee ID cards, TSA to passenger lists and concert and sports venues to ticket purchasers. Such connections should be made in a way that protects personally identifying information whenever possible … Whenever and wherever possible data should be open.”
Are You Ready to Give Up EVERYTHING Over a Virus?
“Privacy concerns must be set aside.” Infection status must be “accessed and validated in a few required settings.”
Infection status will be linked to schools, office buildings, places of work, airports, concert and sport venues — in other words, most areas people need or want to frequent, if not daily, then at least occasionally. Infection status must be known “for people to participate in societal functions.” Legislation must be passed to protect people from being fired from their jobs based on their infection status. Are you concerned yet?
Anyone who remembers the tactics employed in Nazi Germany, or anyone familiar with the current surveillance of the Chinese population, will realize where this is headed.
Reading through the plan, it should also be crystal clear that this tracking and surveillance program is not designed to be temporary. You can be strongly assured this will be permanent. It calls for hundreds of thousands of new employees, updating computer systems and new laws that in many ways resemble the implementation of TSA post-9/11.
Not addressed in this report is the question of just how often would you have to undergo testing. A negative test today may not be valid tomorrow, if you happen to come across someone who is infected between now and then. Would you have to undergo testing every single day? Once a week?
If regular retesting is not part of the plan, then the whole system is worthless as your infection status could change at any time.
Other questions not addressed: If you happen to be in the vicinity of someone who tests positive in the near future, would you have to quarantine for two weeks? Will your employer pay for that time off? Will you have a job when you come out of quarantine?
What if you quarantine for two weeks but don’t get sick and test negative for antibodies, then go out and happen across yet another person who ends up testing positive shortly thereafter. Will you be forced into quarantine again? Where does it end?
The tracking system The Rockefeller Foundation is calling for is eerily similar to that already being used in China, where residents are required to enroll in a health condition registry. Once enrolled, they get a personal QR code, which they must then enter in order to gain access to grocery stores and other facilities.10
The plan also demands access to other medical data. According to the “National COVID-19 Testing Action Plan”:11
“This infection database must easily interoperate with doctor, hospital and insurance health records in an essential and urgent national program to finally rationalize the disparate and sometimes deliberately isolated electronic medical records systems across the country …
Unfortunately, obtaining the necessary clinical data to bring these powerful analytic tools to bear has been difficult due to information-blocking tactics of electronic health records (EHR) vendors. Among the longtime tactics used by such vendors has been charging unreasonable fees for data access, requiring providers to sign restrictive contracts, and claiming patients’ clinical data is proprietary.
On March 9, the Department of Health and Human Services (HHS) released two long-awaited final rules that would prohibit information blocking in health care and advance more seamless exchange of health care data. But publication in the Federal Register, necessary to activate the rules, has been inexplicably delayed. This delay must end.”
In other words, this plan is far more comprehensive than merely tracking COVID-19 cases. It’s designed to replace the current system of “disparate and sometimes deliberately isolated electronic medical records systems across the country.”
ID2020
While The Rockefeller Foundation’s white paper simply calls for the use of a digital “patient identification number” without indicating exactly how you would carry this ID number on your person, Gates has repeatedly talked about the “need” for some sort of implantable vaccine certificate.
In 1999, The Bill & Melinda Gates Foundation donated $750 million to set up Gavi, The Vaccine Alliance.12 Gavi, in turn, has partnered with the ID2020 Alliance, along with the Bangladeshi government, to launch a digital identity program called ID2020.13
The Bill & Melinda Gates Foundation also funded the GSMA Inclusive Tech Lab, launched in 2019, the aim of which is to promote access to digital and biometric identity services and systems.14,15
ID2020, which also launched in 2019, is designed to “leverage immunization as an opportunity to establish digital identity.” This digital identity system is said to carry “far-reaching implications for individuals’ access to services and livelihoods,” so to think that Gates’ call for implantable COVID-19 vaccine certificates would be limited to that alone would again be a grave mistake.
Like The Rockefeller Foundation, Gates is not presenting short-term, temporary measures. They’re both aiming to implement a totalitarian control system. It’s not so far-fetched to imagine a future in which your vaccine certificate or “unique patient ID number” replaces personal identifications such as your driver’s license, state ID card, Social Security card and passport, and is tied not only to your medical records in total, but also your finances.
I remain confident that it would be a tragic mistake to trust Gates, Rockefeller, Google or any of the other players that are being brought before us as the saviors of the day. While most people are well-acquainted with the Rockefeller name, few probably know the true history of the Rockefellers' rise to power. If you fall in this category, be sure to read “How the Oil Industry Conquered Medicine, Finance and Agriculture,” which features an excellent video report by James Corbett.
Those who are ignorant of history are bound to repeat it, and if the Rockefeller story tells us anything, it is that unless we realize what has been done, we'll be deceived again and again, because the oil oligarchy's end game is yet to be realized — if we let them.
from Articles https://ift.tt/2WPk0ZM
via IFTTT