Health, Fitness,Dite plan, health tips,athletic club,crunch fitness,fitness studio,lose weight,fitness world,mens health,aerobic,personal trainer,lifetime fitness,nutrition,workout,fitness first,weight loss,how to lose weight,exercise,24 hour fitness,
Labels
Technology
New Post
[recent][newsticker]
09/24/20
Top Health News -- ScienceDaily
Aging
Alzheimer's
Articles
Articles : Asthma
Articles : CAFO
Articles : Children's Health
Articles : Cholesterol
Articles : Emotional Health
Articles : Fibromyalgia
Articles : GMO
Articles : Heart Health
Articles : Hormones
Articles : Internal Videos
Articles : Interviews
Articles : Men's Health
Articles : Politics
Articles : Thyroid Disease
Articles : Vaccines
Autism
best natural health source
Children's Health
Detoxification
Diabetes
Diet | body+soul
Diet and Weight Loss News -- ScienceDaily
Digestive Diseases
Dite
Dite & weight loss
Drug Industry
Drugs
EFT
EMF
Emotional Health
Finances
fitness
Fitness | body+soul
Fitness/Exercise
Fluoride
Food
Fructose/Sugar
Gardening
Harvard Health Blog
Health
Health | body+soul
Health and Wellness
health news
health tips
Heart Health
information
Joint Support
Juicing
Men's Health
news
Nutrition
Nutrition | body+soul
Pollution
Raw Milk
Soy
Supplements
Swine Flu
Technology
Thyroid Disease
Top Health
Top Health News -- ScienceDaily
Under Armour
Vaccines
Weight Management
women's health
Women's Health News -- ScienceDaily
work place health
Workplace Health News -- ScienceDaily
Fructose made in the brain could be a mechanism driving Alzheimer's disease, researchers propose
New research proposes that Alzheimer's disease may be driven by the overactivation of fructose made in the brain. The study outlined the hypothesis that Alzheimer's is a modern disease driven by changes in dietary lifestyle that has resulted in excessive fructose metabolism in the brain.
from Top Health News -- ScienceDaily https://ift.tt/2RV5ZHE
from Top Health News -- ScienceDaily https://ift.tt/2RV5ZHE
Accuracy of commercial antibody kits for SARS-CoV-2 varies widely
There is wide variation in the performance of commercial kits for detecting antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/34cekgb
from Top Health News -- ScienceDaily https://ift.tt/34cekgb
Talc and petroleum jelly among the best lubricants for people wearing PPE, study finds
Talcum powder, a coconut oil-cocoa butter beeswax mixture, and petroleum jelly provide the best skin protection for long-term PPE use, say scientists.
from Top Health News -- ScienceDaily https://ift.tt/365MeW8
from Top Health News -- ScienceDaily https://ift.tt/365MeW8
COVID-19: Berlin scientists lay basis for a passive vaccination
Researchers have identified highly effective antibodies against the coronavirus SARS-CoV-2 and are now pursuing the development of a passive vaccination. In this process, they have also discovered that some SARS-CoV-2 antibodies bind to tissue samples from various organs, which could potentially trigger undesired side effects.
from Top Health News -- ScienceDaily https://ift.tt/3i1Kwr6
from Top Health News -- ScienceDaily https://ift.tt/3i1Kwr6
Researchers examine COVID-19 impact on manufacturing
A new study finds that manufacturing response to COVID-19 has been largely reactive and uncoordinated, and many firms' crisis communication plans do not include managing an infectious-disease outbreak.
from Top Health News -- ScienceDaily https://ift.tt/330asPJ
from Top Health News -- ScienceDaily https://ift.tt/330asPJ
Job security, finances strongly related to increased anxiety during pandemic
For people still employed during the COVID-19 pandemic, job insecurity and financial concern are associated with greater symptoms of depression and anxiety, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/3kM9X1I
from Top Health News -- ScienceDaily https://ift.tt/3kM9X1I
Variation in genes associated with viral entry of SARS-CoV-2 unlikely to influence COVID-19 morbidity and mortality, study finds
A comprehensive search of genetic variation databases has revealed no significant differences across populations and ethnic groups in seven genes associated with viral entry of SARS-CoV-2.
from Top Health News -- ScienceDaily https://ift.tt/2S9wNEx
from Top Health News -- ScienceDaily https://ift.tt/2S9wNEx
Remote neuropsychology tests for children shown effective, study finds
Administering neuropsychology evaluations to children online in the comfort of their own homes is feasible and delivers results comparable to tests traditionally performed in a clinic, a new study indicates. The finding could help expand access to specialists and reduce barriers to care, particularly as the popularity of telemedicine grows during the COVID-19 pandemic.
from Top Health News -- ScienceDaily https://ift.tt/3i23jTs
from Top Health News -- ScienceDaily https://ift.tt/3i23jTs
Some severe COVID-19 cases linked to genetic mutations or antibodies that attack the body
Two new studies offer an explanation for why COVID-19 cases can be so variable. A subset of patients has mutations in key immunity genes; other patients have auto-antibodies that target the same components of the immune system. Both circumstances could contribute to severe forms of the disease.
from Top Health News -- ScienceDaily https://ift.tt/303SWrY
from Top Health News -- ScienceDaily https://ift.tt/303SWrY
Mapping the human heart, cell by cell
Scientists have mapped and described the function of cells in six regions of the adult heart, providing a new foundation for studying heart disease.
from Top Health News -- ScienceDaily https://ift.tt/3cvz71D
from Top Health News -- ScienceDaily https://ift.tt/3cvz71D
Uncovering a 'suPAR' culprit behind kidney injury in COVID-19
A new observational study finds patients in the hospital for COVID-19 have high levels of soluble urokinase receptor (suPAR), an immune-derived pathogenic protein that is strongly predictive of kidney injury.
from Top Health News -- ScienceDaily https://ift.tt/3mLi0Op
from Top Health News -- ScienceDaily https://ift.tt/3mLi0Op
New tool mimics human skin to allow detailed study of mosquito biting
Scientists have developed a tool for studying the biting behavior of common pathogen-carrying mosquitoes.
from Top Health News -- ScienceDaily https://ift.tt/3kD7Xce
from Top Health News -- ScienceDaily https://ift.tt/3kD7Xce
Placenta is initiated first, as cells of a fertilized egg divide and specialize
The first stages of placental development take place days before the embryo starts to form in human pregnancies. The finding highlights the importance of healthy placental development in pregnancy, and could lead to future improvements in fertility treatments such as IVF, and a better understanding of placental-related diseases in pregnancy.
from Top Health News -- ScienceDaily https://ift.tt/307vSIO
from Top Health News -- ScienceDaily https://ift.tt/307vSIO
Lifestyle medicine for all: Healthy food comes first
“Lifestyle medicine is only for rich people, right?” a colleague asked me several years ago, questioning my involvement in this relatively new field of medicine that guides people toward healthy habits. This has been a common misperception, for sure.
But across the US, a revitalized brand of health activism is intent on bringing lifestyle medicine to a broader range of people. This is backed by a new effort from the American College of Lifestyle Medicine to engage communities most affected by chronic disease.
The first pillar of healthy lifestyle: Food is medicine
Lifestyle medicine is an evidence-based practice of helping people adopt and sustain healthy behaviors like improving diet, increasing activity, managing stress, sleeping well, moderating alcohol consumption, and quitting tobacco. Large studies show such habits can extend our lives by well over a decade. What’s more, these habits can even keep these extra years free of diseases like diabetes, heart disease, strokes, and cancer.
Eating a plant-based diet — meaning a diet rich in vegetables, fruits, beans and legumes, nuts and seeds, and whole grains — can lower inflammation, as well as the risk of many chronic diseases such as diabetes, heart disease, strokes, and cancer. Simply put, food is medicine. Some doctors are providing this information to patients as part of their regular medical care.
But many people do not have easy access to healthy plant foods. Especially now, they may be suffering from significant financial limitations, unemployment, and unstable housing. Or they may live in a “food desert,” where grocery options are severely limited, or worse, a “food swamp,” an area where fast food and junk food are more available than anything else. Living in a food swamp puts people at a higher risk of becoming overweight or obese.
Ways to help change the equation
Helping patients access healthy plant foods is critically important. And some doctors and academic medical centers are taking action to bring healthy foods to underserved communities.
Food pantries. Dr. Jacob Mirsky is a physician at Massachusetts General Hospital and co-director of the department of medicine’s Healthy Lifestyle Program. He works in an underserved community north of Boston, where he directs his clinic’s new plant-based food pantry. When he prescribes a plant-predominant diet to his patients, he also is able to provide the plants. He views this work as activism and a potent way to address inequalities while also taking care of his patients.
Plant-based food pantries and food prescription programs have been positively received by communities. One such program in a rural, low-income area of Texas provided 30 pounds of fresh produce to households identified as food-insecure — meaning they did not have enough food to eat — every two weeks for six months. Participants described the program as critical for helping them feed their families, and 99% reported that they consumed all or almost all of the food they received.
Education and support. Dr. Michelle McMacken is an assistant professor of medicine at New York University’s Grossman School of Medicine, and director of the Plant-Based Lifestyle Medicine Program at NYC Health and Bellevue Hospital. She is working to make lifestyle medicine services available to as many patients as possible, regardless of socioeconomic status.
“I believe everyone deserves access to lifestyle medicine, especially the highest-risk, most vulnerable patients who potentially stand to benefit the most,” she says. “The majority of my patients — including those facing significant socioeconomic challenges — want to learn what they can do to become healthier. We collaborate to figure out how they can leverage lifestyle medicine within their own situation.”
Despite challenging circumstances, she has seen patients achieve health transformations, including weight loss and improved cholesterol and blood sugar levels.
Programs that educate people about the power of plant foods can have a big impact. A study of 32 Latinx people with type 2 diabetes living in a medically underserved area of California offered a five-week program introducing participants to the power of plant foods. Declines in blood sugar continued even six months after that program had ended.
Connecting people and food. The Family Van is a longtime mobile health program supported by Harvard Medical School that provides free education, resources, and some clinical services to anyone, regardless of insured status. A large part of what they do is help people access nutritional support through SNAP (Supplemental Nutrition Assistance Program) and locate low-cost produce sources like The Fresh Truck and The Daily Table. They also will provide grocery gift cards along with their healthy diet counseling. The Family Van has been collecting data such as body mass index, blood pressure, blood sugars, and ore for over a decade, and has published several papers showing that such interventions work.
Programs like these are essential and wonderful, but there is a lot more work to be done. In our Healthy Lifestyle Program at Massachusetts General Hospital, we hope to establish the practice of healthy lifestyle as the standard of care for preventing and treating chronic disease for all of our patients. To do this, we are developing practical, accurate methods to assess clinically important diet and lifestyle factors at every patient’s physical exam. At the same time, we’re studying evidence-based approaches to help people eat and live healthier, including our plant-based food pantry, health coaching, and web-based group education classes. We hope that in the future, every one of our patients will have access to the quality information, resources, and support that they need to live their healthiest life.
The post Lifestyle medicine for all: Healthy food comes first appeared first on Harvard Health Blog.
from Harvard Health Blog https://ift.tt/33ZOICQ
New brain cell-like nanodevices work together to identify mutations in viruses
Scientists have described a new nanodevice that acts almost identically to a brain cell. Furthermore, they have shown that these synthetic brain cells can be joined together to form intricate networks that can then solve problems in a brain-like manner.
from Top Health News -- ScienceDaily https://ift.tt/2G5iw92
from Top Health News -- ScienceDaily https://ift.tt/2G5iw92
New mechanism of action against SARS-CoV-2 by antiviral drug remdesivir
Researchers have discovered a novel, second mechanism of action by the antiviral drug remdesivir against SARS-CoV-2. The research team previously demonstrated how remdesivir inhibits the COVID-19 virus's polymerase or replication machinery in a test tube.
from Top Health News -- ScienceDaily https://ift.tt/3cpZ9Uf
from Top Health News -- ScienceDaily https://ift.tt/3cpZ9Uf
Irena wins Locky Gilbert’s heart!
The winner of this year's The Bachelor has been announced, with Irena Srbinovska whisking Locky Gilbert's heart away.
from Health | body+soul https://ift.tt/3cvrB7g
from Health | body+soul https://ift.tt/3cvrB7g
NVIC's 2020 Annual Report on US State Vaccine Legislation
Over the last decade, there has been a significant increase in vaccine related legislation that impacts every person.
More vaccines have been mandated for children in school and daycare and adults in the workplace, vaccine exemption rights have been restricted or removed, emergency powers have been expanded, vaccine tracking and enforcement and vaccine exemption rate disclosure programs threaten choices and health outcomes, and parental and informed consent rights have been weakened or removed all together.
This has all happened under the backdrop of unprecedented censorship of information questioning the safety, efficacy or necessity of the dozens of vaccines being mandated for use and the hundreds of vaccines in development.
Public shaming, marginalization and the bullying of those who don’t agree with accepting every single dose of every federally recommended and state mandated vaccine has become not only commonplace but socially sanctioned by those promoting “no exceptions” vaccine policies and laws.
In addition, with the declaration of a COVID-19 pandemic in March 2020, plans to roll out a national vaccination program loom on the horizon. If the COVID-19 vaccine becomes state mandated, it has the potential to alter life in America in ways we never thought could be possible.
Citizen involvement in the legislative process to protect the human right to exercise informed consent to vaccination increased to unprecedented levels in 2020. In many cases, it matched and overcame the relentless attack by mandatory vaccination proponents on the ability of individuals to decline vaccination.
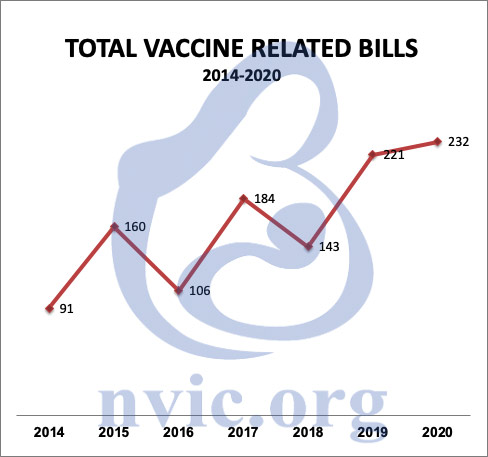
Highest Number of Vaccine-Related Bills in NVIC’s History
In this 2020 Annual Report on U.S. State Vaccine Legislation, the non-profit educational charity National Vaccine Information Center (NVIC) reports that during the 2020 legislative session, NVIC analyzed, tracked and issued positions on an unrivaled 232 vaccine related bills in 39 states and the District of Columbia through the NVIC Advocacy Portal.
This was the highest number of bills in the history of NVIC’s advocacy program, despite many shortened state legislative sessions due to COVID-19 social distancing restrictions.
Working to prevent vaccine injuries and deaths through public education since 1982, NVIC is the largest and oldest U.S. consumer-led non-profit organization disseminating information about diseases, vaccines and informed consent to vaccination.
NVIC provides well-referenced, accurate information to the public about vaccine science, policy and law but does not make vaccine use recommendations. In 2010, NVIC launched the NVIC Advocacy Portal (NVICAP), a free online vaccine choice advocacy network, for the purpose of securing and defending informed consent protections in vaccine policies and laws.
Over the last decade, the NVIC Advocacy Program has analyzed, tracked and issued positions on well over 1000 vaccine related bills and has worked alongside and shares legislative information with many health freedom groups that support NVIC’s almost four-decade call for the protection of vaccine informed consent rights in America.
The NVIC Advocacy Portal team, including key NVIC Advocacy directors in many states, works with families and enlightened health care professionals to educate legislators and protect vaccine informed consent rights. NVIC issues action alerts and sends them through email, posts them online and shares them through social media and our text alert program.

>>>>> Click Here <<<<<
At the time this report was prepared, vaccine-related bills are still pending in California, District of Columbia, Illinois, Massachusetts, Michigan, New Jersey, New York, Ohio, Pennsylvania, Virginia, Vermont, and Wisconsin.
Action to support the good vaccine-related bills and oppose bad bills is still needed. Bills referenced in this report are published on the NVIC Advocacy Portal and registered users can obtain a more detailed bill analysis, including current status, NVIC’s position on the bill, and recommended action.
Highlights From 2020
There were significant positive take away points from the outcome of the 2020 legislative session:
|
13 bills in 10 states [CT, FL, IA, IL, MA, NJ, PA, VT, WA, WI] were filed to eliminate vaccine exemptions. None passed. |
|
Out of 10 bills filed across eight states [CO, FL, MA, NJ, NY, OK, PA, VT] to restrict vaccine exemptions, only one passed. Colorado SB 163 requires a vaccine provider signature or the completion of an online re-education module for religious or conscientious exemptions. |
|
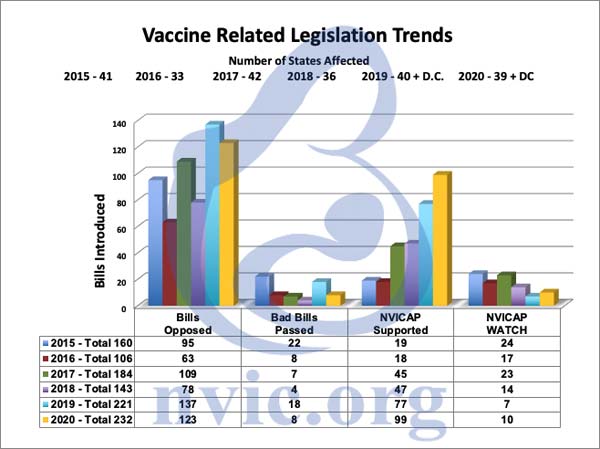
Out of the 123 vaccine-related bills that NVIC opposed, only eight bad bills passed! |
|
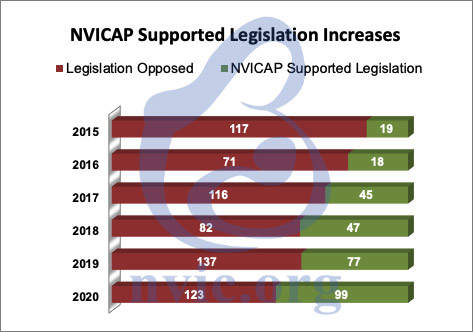
The 2020 legislative session featured 99 bills worthy of NVIC’s support, which is more than any legislative session since the launching of NVIC’s Advocacy Portal in 2010. This is up from only 18 good bills NVIC supported in 2016. The ratio of the total bills supported compared to total bills opposed has gotten better and better. Two of these positive bills passed. |
|
Proposed administrative rules to either add vaccine mandates or restrict exemptions in four state that NVIC opposed were withdrawn or amended to take out the offending sections. |
|
There were only three states with more than 10 vaccine related bills filed in the 2020 session. Iowa led states in most positive bills introduced with 16 bills worthy of support and only three that required opposition. New Jersey had four bills worthy of support and 13 deserving opposition. The informed consent rights of New Yorkers were attacked by more bills than any other state with 27 bills needing opposition and only eight that deserved support. |
The remaining vaccine-related bills for the 2020 session are broken out and described below by category.
2020 Bill Analysis by Category
The four main areas that NVIC focuses on when tracking proposed bills are:
- Vaccine exemptions and informed consent rights
- Vaccine mandates
- Vaccine tracking and reporting
- Vaccines in general
Some bills may be included in multiple categories. For example, a proposed bill attempting to mandate a vaccine may also have a requirement for vaccine tracking so it would be counted in both categories but only counted once in the total bill count.
The NVIC Advocacy team provides referenced, accurate vaccine information and talking points for NVICAP users to background legislators. Some of the position statements NVIC posted on the Advocacy Portal in 2020 were listed as bills to “watch.”
This is done because our analysis indicated that either the bill was well intentioned but contained some problems needing amending before we could support it or the bill contained sections that were highly vulnerable to amendments that could conflict with NVIC’s mission.
The breakout and analysis of bills in these different categories identifies trends across the states and serves as a guide if you want to become active by joining the NVIC Advocacy Portal and educating your state legislators and community in 2021 about why it is so important to protect vaccine informed consent rights.
Vaccine Exemptions and Informed Consent (138 Bills)
In a positive turnaround from previous sessions, out of the 138 vaccine-related bills filed in state legislatures in 2020 having components affecting vaccine exemptions and informed consent rights, NVIC opposed 56 of the proposed bills, but supported 78 and “watched” four. This is the first session where NVIC has supported more exemption and informed consent bills than opposed.
The mainstream media tended to hype the bills attacking exemptions so much that it may come as a surprise that there were more bills to expand exemptions and informed consent rights than there were to eliminate or restrict those rights.
This can be directly credited to positive action taken by forward thinking state legislators, who were given fact-based information about vaccines, exemptions, and diseases by concerned citizens who took the time to make one-on-one personal contact with their elected representatives.
Eliminating or Restricting Vaccine Exemptions
There was a noticeable drop in bills filed in 2020 to either remove or restrict exemptions: 23 in 2020 versus 40 in 2019. There were 13 bills in 10 states (Connecticut, Florida, Iowa, Illinois, Massachusetts, New Jersey, Pennsylvania, Vermont, Washington and Wisconsin) that were filed to eliminate vaccine exemptions. None passed.
Notable in these defeats was Connecticut HB 5044 attempting to remove the religious exemption, which broke all records for online testimony that gripped the country overnight and lasted over 21 hours into the next morning. This bill did not pass.
Florida SB 64 to remove the religious exemption was filed by Senator Lauren Book in 2019 before the 2020 legislative session even started. This prompted families around the state to fight back by attending local pre-session delegation meetings asking for the bill’s defeat.
Health Freedom Florida hosted a rally featuring presentations by NVIC and Children’s Health Defense the first week of session to educate citizens about the bill. This proactive strategy was effective. SB 64 failed to pass and did not even get a hearing.
New Jersey’s religious exemption removal bills (A969/S902) drew more in person protests than any vaccine bill had done before with many thousands showing up to oppose the exemption removal. Legislators inside the capitol building could hear protesting parents chanting for hours outside. This bill came the closest to passing of all the exemption removal bills. The strong showing by New Jersey families helped provide support to the brave legislators opposing this bill.
Out of 10 bills filed across eight states (Colorado, Florida, Massachusetts, New Jersey, New York, Oklahoma, Pennsylvania and Vermont) to restrict vaccine exemptions, only one passed. Colorado SB 163 requires a vaccine provider signature or the completion of an online re-education module for religious or conscientious exemptions.
Bills pending to remove or restrict vaccine exemptions that deserve continued strong opposition are still active in Illinois, Massachusetts, New Jersey, New York, Pennsylvania, and Vermont. These bills need to continue to be opposed.
It is critical that vaccine choice advocates in every state register for and regularly check in to the NVIC Advocacy Portal. The most important thing you can do if you care about this issue is to establish relationships with and educate your legislators now and into next year so you can be ready to counter bills that will restrict or eliminate exemptions and get good bills filed to protect and expand vaccine exemptions.
There is nothing more important that you can do to protect or expand your right to delay or decline vaccines without penalty or harassment than talking to your legislators in person and establishing a positive, respectful relationship with them.
Exemption Disclosure and School Shaming
The trend to publicly disclose vaccine exemptions to shame schools with higher exemption rates has continued in 2020 where nine bills were filed in seven states. This year none of these bills passed.
Promoted by those who seek to ultimately eliminate vaccine exemptions, these public disclosure bills threaten and place pressure on students with vaccine exemptions by requiring schools to publish vaccination and/or vaccine exemption rates online.
These bills are promoted under the false pretense of transparency, but they are really about government-sponsored shaming of schools with students who have vaccine exemptions.
The real goal of school shaming bills is to create centralized repositories of specific community level vaccine usage data that the media and public health employees use to identify and locate those who decline to receive every vaccine recommended by the CDC’s Advisory Committee on Immunization Practices.
Media will use these reports in a biased manner to reflect negatively on schools with more exemptions in an attempt to solicit support for further restricting or eliminating vaccine exemptions.1
Setting up schools to be designated “winners” and “losers” in the myopic quest for a 100 percent vaccination rate with all federally recommended vaccines, these types of bills add more layers of pressure and coercion with every single dose of every single vaccine and create an environment that pits parents, children, schools and districts against each other.
Arizona has had a bill filed every year since 2015 to post vaccine exemption rates. Fortunately, they have all failed to pass thanks to proactive citizen advocacy and brave legislators, who have held back these bills from moving forward.
Even though these bills don’t authorize the release of individually identifiable information, the numbers of children utilizing vaccine exemptions are so small that bills like these puts the exposure of children’s identity at risk and sets them up for harassment, discrimination, and bullying. These bills need to continue to be opposed.
Children Vaccinating Themselves?
A very troubling area of proposed legislative changes are bills that allow minor children to be vaccinated without the knowledge or informed consent of their parents. A child is less likely than an adult parent to understand their personal and family medical history, including a history of vaccine reactions, allergies and autoimmune or neurological disorders.
Minor children do not have the same kind of critical thinking skills or emotional maturity required to make a vaccine benefit-risk decision compared to an adult. In addition, if a child receives a vaccination without a parent’s knowledge or informed consent and then experiences a vaccine reaction, a parent might not recognize the potential cause of their child’s sudden decline in health.
This lack of knowledge by parents could be life threatening for the child. None of the 21 bills introduced in eleven states (Colorado, Georgia, Illinois, Massachusetts, Maryland, New Hampshire, New Jersey, New York, Virginia, Vermont, Wisconsin and the District of Columbia), which attempted to grant minor children the ability to consent to vaccines on their own without parental knowledge or consent, passed.
In 2019, Congress held two vaccine hearings, one on February 27th2 and another on March 5th3 and one focus of the hearing pitting children against their parents.
Veteran vaccine safety and informed consent advocates with nearly four decades of experience, including time spent serving on federal advisory committees, were denied the ability to testify, but a teenager with no experience other than recently opposing his mother on social media4 for not vaccinating him was invited to testify.5
The ill-conceived concept of minor children consenting to vaccination without their parents’ consent appeared in media6 stories more frequently following the congressional hearing and used the teen’s testimony to advocate for this policy change.
Medical trade groups also advanced the concept. Doctors, who are frustrated with having to spend time talking with educated parents during routine “well child” visits to answer questions and concerns about vaccines, have identified minor consent as a way to coerce children into consenting to vaccines on their own.
Adolescents are vulnerable to peer and authority-figure persuasion. An opinion piece was published in The New England Journal of Medicine7 and the American Medical Association passed a resolution8 supporting state laws to allow minors to consent to vaccination.
This coordinated effort resulted in 13 bills introduced in 2019 and a big jump to 21 bills introduced in 2020. Fortunately, legislators listened to parents and rejected all 34 minor consent bills filed in 2019 and 2020. Federal legislative history provides evidence that Congress never intended for a minor child to make decisions to get a vaccine without parental knowledge or consent.
When the National Childhood Vaccine Injury Act9 of 1986 was passed, the Act clearly stated that before the administration of certain vaccines,10 a health care provider shall give a copy of the CDC’s vaccine information materials to either the, “the parent or legal representative of any child to whom the provider intends to administer such vaccine …”
The CDC asserts the requirement that the VIS sheet is provided to the parent/legal guardian prior to vaccination of a minor child on their Q&A page on VIS sheets:11 Under the question “Is there a requirement to verify that parents/legal representatives have actually received and reviewed the VIS,” the answer is a clear and undebatable “YES.”
There is no justification for the state to override a parent’s legal right to make an informed benefit and risk decision about vaccination on behalf of their minor children and hand that legal right to doctors and medical workers, who have no liability or accountability for what happens to the child after vaccination.
These types of bills are a violation of parents’ constitutional right to raise their children without undue interference from the state, and each one of these bills that surfaces in state legislatures should be strongly opposed.
Expanding Vaccine Exemptions and Informed Consent
Hard working vaccine and health freedom advocates and open-minded legislators came together in 2020 to advocate for 78 bills in the following 25 states to expand vaccine exemptions and enhance informed consent rights:
|
Arizona |
California |
Colorado |
|
Delaware |
Florida |
Georgia |
|
Illinois |
Iowa |
Louisiana |
|
Michigan |
Minnesota |
Mississippi |
|
Missouri |
New Jersey |
New York |
|
Ohio |
Oklahoma |
Oregon |
|
Pennsylvania |
Rhode Island |
South Carolina |
|
Tennessee |
Vermont |
Washington |
|
West Virginia |
This is a big jump from the 58 bills of this kind filed in 2019. In response to expanding vaccination schedules and overzealous forced vaccination polices implemented by day care and schools, legislators filed 20 bills in the following 12 states to expand vaccine exemptions:
|
Delaware |
Iowa |
Louisiana |
|
Minnesota |
Missouri |
Mississippi |
|
New York |
Rhode Island |
South Carolina |
|
Tennessee |
Washington |
West Virginia |
Most of the bills filed added religious or conscientious exemptions. While no bills adding vaccine exemptions for children to attend daycare and school were passed, Delaware passed a bill (HB 214) to allow veterinarians to exempt animals from rabies vaccines if the veterinarian concludes the vaccine would endanger the animal’s health.
Gaps in Informed Consent on Legislators’ Radar to Fix
Legislators are increasingly recognizing problems created because parents are not provided enough information about potential vaccine risks and contraindications.
In response, 30 bills were filed in 16 states tackling the issue of improving vaccine informed consent rights. California, Colorado, Georgia, Iowa, Illinois, Louisiana, New Jersey, New York, Ohio, Oklahoma, Pennsylvania, Tennessee, Vermont, Washington, and West Virginia all had bills filed to require additional information to be provided prior to vaccination.
Nine states had legislators wanting to get better information about the increased prevalence of vaccine reactions. 11 bills were filed to require vaccine reactions to be reported to the legislature directly or through a state agency. Iowa, New Hampshire and Missouri each had a bill introduced to require death certificates to include information about vaccines administered.
Also addressing gaps in informed consent, 9 bills were filed in the 7 states of Colorado, Florida, Iowa, Louisiana, Ohio, Oklahoma, and Pennsylvania that would require parents to be informed of the availability of vaccine exemptions. Often, parents do not know they have the legal right to take a vaccine exemption.
Some schools don’t readily share this information and parents may be incorrectly told there is a “no shots, no school” policy that prevents unvaccinated or partially vaccinated children from enrolling in school. This can result in a child, who may be at high risk for suffering a vaccine reaction, getting vaccinated under false pressure that can lead to the child suffering a serious reaction.
Other bills filed required the disclosure of certain vaccine ingredients and risks, and several bills added steps like requiring specific written permission before any vaccine could be administered. One broad groundbreaking bill in Florida entitled the “Stop Social Media Censorship Act,” would have provided civil remedies for those whose religious or political speech was censored by a social media website.
While none of these bills passed, over 1,000 state legislators were educated about the failures in the informed consent process to vaccination. This education can serve as a deterrent to passing other bad bills that remove or restrict informed consent rights from being introduced in the future.
Decreasing Discrimination
An encouraging new trend is that more legislators are recognizing the significant problems caused by discrimination against those who choose to delay or decline vaccination and are willing to support legislation to stop this discrimination and bias.
A total of 32 bills tackling different aspects of discrimination head on were filed. The majority of bills filed were trying to protect adult employees from any kind of penalties for refusing vaccines. This category of bills will be extremely important in 2021 as COVID-19 vaccines are rolled out and potential legislation is introduced to mandate COVID-19 vaccinations.
It is critical to protect people from sanctions by employers, insurance companies, medical providers, retail establishments, and interstate travel opportunities for refusing to take a vaccine. It is not too early to talk to legislators about prefiling bills to prevent this type of discrimination ahead of the 2021 legislative session.
Six bills were introduced this session to specifically prohibit insurance companies from penalizing doctors or patients when the patient did not take a recommended vaccine, while one bill in Wyoming prohibited doctors from expelling patients for vaccine refusal, and another Wyoming bill prohibited hospitals from refusing to treat individuals based solely on their vaccination status.
Iowa and Michigan filed bills that would prohibit denying a foster care license based on the vaccination status of the family. Arizona, Colorado, and Oregon also tried to join the ranks of Texas with bills that prohibit either abuse claims or custody restrictions based on vaccine refusal, and Colorado’s efforts were rewarded with the passage and governor’s signature on HB 1297.
This clarified that delaying or declining a vaccine by itself is not child abuse or neglect. This bill enjoyed notable bipartisan support. Colorado demonstrated that it is important not to prejudge legislators based on party affiliation for their support or opposition to a bill and it is important to sincerely educate and treat all legislators respectfully.
Expanding Vaccine Mandates
In 2020, only three of the 42 bills filed to add vaccine mandates passed. Two bills were in New Jersey. Annual flu vaccines are now required for health care facility employees in New Jersey and meningococcal vaccines are now mandated for residential students at four-year colleges in New Jersey.
The third and worst vaccine mandate bill to pass in 2020 was Virginia HB 1090. It gave the Governor-appointed Board of Health the authority to add federally recommended vaccines to the schedule required for school attendance (with the exception of requiring annual influenza vaccinations) without a public hearing or vote by the legislature.
It also expanded the current list of required vaccines to add HPV vaccines for boys to the existing requirement for girls and added rotavirus, hepatitis A, and meningococcal conjugate vaccine requirements in conformance with recommendations of the CDC’s Advisory Committee on Immunization Practices (ACIP).
This puts Virginia school children at risk of being required to receive a mandated COVID-19 vaccine once it is licensed by the FDA and recommended by ACIP for children. The Health Commissioner of Virginia has already stated that he intends to mandate12 that all Virginians get a COVID-19 vaccine when it is available.
Mississippi had a failed attempt to pass a bill to mandate annual flu vaccines for school employees with no religious exemption, and New York still has two pending bills attempting to mandate flu vaccines for children in school and daycare, A2316 and S2776, that need to be watched and opposed.
Five states — Illinois, Massachusetts, New Jersey, New York and Virginia — had bills filed to specifically mandate HPV vaccines for students that have not passed. New Jersey, New York, and Ohio attempted to add other adult vaccine mandates. NVIC opposes all adult mandates as a condition for employment. Vaccines are already available to those who want them.
New York attempted a bill to mandate vaccines for children’s camps with no religious exemptions allowed, but it has not passed.
Restricting Vaccine Mandates
NVIC supported 20 bills in 13 states that would have restricted vaccine mandates. While none of these bills passed, many legislators were educated about the harm vaccine mandates can cause, and this education helped hold back the passage of dozens of bills enacting more forceful mandates.
Eight bills were filed in Colorado, Idaho, Louisiana, Michigan, Minnesota and Ohio to protect employees who want to refuse vaccination requirements. These types of bills need to be filed and passed in every state.
Michigan had two bills, HB 5135 and HB 5136, that would have prohibited new vaccine mandates to be issued by agency rule making. Oklahoma passed a bill in the House, but not the Senate, to require legislative approval when new vaccine mandates are added for school by the department of health.
Given the threat posed by unelected and unaccountable state employees having the power to expand vaccine mandates, lawmakers in state legislatures, who have punted the responsibility of setting the vaccine schedule to health agency employees, need to take their legislative authority back so the people these mandates affect have a voice and can participate in the democratic process.
Iowa and Michigan set their sights on prohibiting a requirement that foster care families vaccinate their families. While the Iowa bill died, the Michigan bill is still pending, and support could help tip this good bill over the edge to pass.
Two exciting bills were introduced in Arizona (HB 2050) and South Dakota (HB 1235) to eliminate vaccine mandates, and people should consider talking to their legislators about filing this kind of bill in their own states.
Brave legislators in these states recognized that vaccines are pharmaceutical products that can cause injury or death, and families should be allowed to make voluntary decisions about their use without being coerced and forced by law to vaccinate. These bills were filed as a direct result of people talking to their legislators about the harm that vaccine mandates have caused their families.
Vaccine Tracking and Reporting (37 Bills)
Forced inclusion, forced reporting, and opt-out electronic vaccine tracking registries and enforcement systems continue to threaten the medical privacy of citizens and their legal right to refuse federally recommended vaccines without being subjected to harassment or punishment.
On the positive side, legislators are also becoming increasingly concerned about the lack of reporting and tracking of serious vaccine reactions and are trying to take steps to put this information in front of more government officials.
The 2020 legislative session included 37 bills in the category of vaccine tracking and reporting that NVICAP analyzed, posted and monitored.
Expanding Vaccine Tracking
Eighteen bills tried to expand vaccine tracking in Alabama, Arizona, Colorado, Indiana, Massachusetts, Nebraska, New Jersey, New York, and Washington. Three of these bad bills passed. This is a big improvement from 2019 where nine bills expanding vaccine tracking passed.
Colorado passed SB 163 which, in addition to restricting vaccine exemptions, adds a hefty dose of increased vaccine tracking and electronic surveillance. Health care providers are required to submit all vaccines administered and also all vaccine exemption information to the state operated electronic vaccine tracking system, CIIS.
Now, there is no way for public and private school students and children attending daycare to not be tracked by the health department in Colorado. Indiana passed HB 1210, which expands the current vaccine tracking system in Indiana to include additional personal health information, including newborn screening and blood lead screening.
Nebraska passed LB 1183, which enacted government vaccine tracking through the Population Health Information Act. The bill was initially introduced to deal with prescription drug monitoring, but it was amended to include vaccine tracking in this new state electronic database.
There is no requirement for opt-in informed consent to participate in this registry and the bill provides for any health care entity to access this information. Alabama, New Jersey and West Virginia had four additional bills that would have required vaccine providers to report to the registry, but fortunately they did not pass.
All 50 states now have vaccine tracking systems13 for children and many states have expanded their systems to include adults. The Centers for Disease Control (CDC) has created a new term for vaccine tracking, surveillance, and enforcement registries so people don’t focus on and become concerned about how they are actually being used.
Threats Posed by Immunization Information Systems
The CDC now calls them Immunization Information Systems (IIS),14 which makes them seem to be more passive and less threatening. In reality, IIS represent one of the largest threats to being free to refuse any vaccination, including upcoming vaccines for COVID-19.
Federal agencies are working with public health trade groups to link the registries all together15 to be able to create and access a complete personalized vaccine profile on every U.S. citizen. The Network for Public Health Law16 recently held two webinars about data sharing to support each “jurisdiction’s role in mass vaccination for COVID-19” using the Immunization (IZ) Gateway.17
The IZ Gateway is sponsored by the CDC Immunization Information Systems Support Branch and led by the U.S. Department of Health and Human Services Office of the Chief Technology Officer.
Its purpose is to facilitate the sharing of everyone’s immunization status through multiple private and government entities in real time to create a virtual national immunization registry so that wherever you are, government and health care providers will know your vaccination status.
This presents a huge problem for people who don’t want to have their vaccination status tracked by government or anyone else. Many states have mandatory tracking where consent is unfortunately assumed and there is no way to get out.
This is sometimes initiated with the state sharing birth records to the immunization registry without a parent’s knowledge or consent for the purpose of initiating a registry file on every newborn. Some states automatically put everyone in the system but claim someone can either opt-out, or opt-out of data sharing.
This is problematic for two reasons. First, because of data interoperability, every system that has access to each state registry can pull an individual’s vaccination status, store it, and release it even further before someone may have a chance to opt-out. Even if someone opts-out, the data is already out there and can’t be taken back.
Second, opting-out of data sharing does nothing to protect your vaccination status from the health department who operates the registry itself. It only prevents other entities like insurance companies, health care providers or schools from accessing the information. This does little to reassure people who are concerned the information will be used to force vaccination.
Many people are more concerned about what public health officials will do with this information now and in the future as the vaccine records in most IIS can never be removed. The only way to guarantee your vaccination status won’t get tracked in existing vaccine tracking registries by your state and used to penalize you or enforce vaccination is for your state to legislate explicit opt-in consent for inclusion into the registry and for the release of data out of the registry.
Also, the option for complete personal vaccine data purging from the registry and all other health department files should be enacted for those who want their personal information removed from the registry after it has been included.
Texas and Montana are the only states that require opt-in informed consent.18 If you do not live in either of these states, laws need to be changed to prohibit any collection or sharing of your medical/vaccine records without your expressed written informed consent. With impending controversial COVID-19 mass vaccination programs, limiting personal health information that is collected and shared with IIS is critical.
Strong opposition to mandatory inclusion, assumed consent, and opt-out vaccine tracking systems is needed. Reaching a 100% vaccine compliance rate by all children and adults is the goal of these electronic vaccine tracking systems.
Expanding Vaccine Reaction Reporting and Tracking
On the other side in a positive new trend, there were 14 bills requiring the reporting or recording of vaccine reactions. California, Iowa, Louisiana, New Hampshire, New Jersey, Rhode Island, Vermont and Washington had 11 bills requiring that reports of vaccine reactions be sent to the legislature or the state.
Iowa, New Hampshire and Missouri took on the heart wrenching topic of infant deaths following vaccination and had three bills requiring vaccine information to be recorded on death certificates or to be reported to the Vaccine Adverse Event Reporting System (VAERS).
While none of these bills passed, legislators were educated about the lack of public transparency about real vaccine reactions and deaths and these bills were a great first step at trying to change that.
Emergency Powers
Arizona and Pennsylvania had two bills that attempted to expand emergency powers by the state but they did not pass. In 2021, we can expect many more bills trying to expand emergency powers, as well as curtail abuses of emergency powers, in direct response to the COVID-19 pandemic of 2020. These bills will need to be watched carefully.
Most states lack sufficient vaccine exemptions to protect citizens from forced vaccination in times of declared public health emergencies. Now would be a good time for people to review their state emergency powers laws to look for problems and talk to their legislators about filing bills before the 2021 legislative sessions to expand vaccine exemptions for all state residents during a declared public health emergency.
This is especially important for those who have concerns about potential mandates for COVID-19 or influenza vaccines.
Authorizing More Professions to Administer More Vaccines
One of the most successful areas where we worked with families in the states was in the area of bills that proposed to expand the authority to pharmacists and others to administer vaccines to children.
There were 22 bills filed in 14 states (Arizona, California, Florida, Iowa, Louisiana, Maryland, New Hampshire, New York, Ohio, Oklahoma, Pennsylvania, South Carolina, Virginia and Wisconsin) to allow pharmacists and other types of medical professions to administer vaccines to young children.
Four of the 22 bills attempted to expand vaccine administrators to other professions outside of pharmacists. Ohio had a bill trying to allow podiatrists to give flu vaccines to anyone 7 years old and up, Oklahoma tried to get paramedics to give vaccines, and Wisconsin tried to give authority to dentists to administer vaccines.
Fortunately, none of these bills passed but it is easy to see how other professions want a piece of the almost $18 billion U.S. vaccine market in 2020,19 and how that could lead to more “gatekeepers” instituting policies that refuse services to the unvaccinated.
In terms of expanding a pharmacist’s ability to give vaccines, both New Hampshire and New York passed controversial futuristic bills allowing pharmacists to vaccinate for COVID-19 once a vaccine becomes available.
Other than the two COVID-19 expansions bills, the only other bill of this type that passed was in Florida, but the offending language allowing pharmacists to vaccinate children was completely removed from the bill thanks to strong opposition.
Unfortunately, the federal government stepped in and overrode the states on the issue of pharmacists being given the authority to vaccinate young children. State legislatures were completely circumvented by an action taken by the Secretary of Health and Human Services, Alex Azar.20
On August 24, 2020, the Federal Register published Mr. Azar’s amendments21 to the declared emergency for COVID-19 issued under the Public Readiness and Emergency Preparedness (PREP) Act for Medical Countermeasures Against COVID-19.
Countermeasures include vaccines for ACIP-recommended vaccines and this amendment now allows pharmacists to administer every ACIP-recommended vaccine to all children 3 years old or older, regardless of what each state law limits. This is a significant abuse of federal power.
Pharmacists Are Not Doctors
States have been deliberately cautious about limiting the types of vaccines and ages of children which pharmacists are allowed to vaccinate. The actions of Mr. Azar, who is a former CEO of the U.S. pharmaceutical company Eli Lilly, and a former pharmaceutical lobbyist,22 illustrate the problems created by the revolving door between the pharmaceutical industry and government agencies.
Pharmacists administering vaccines in the corner drug store or grocery store pharmacy to minor children and toddlers trivializes very real vaccine risks and the potential for serious reactions.
Pharmacists are not doctors and 20 hours of required training23 for pharmacists to be able to administer all childhood vaccines cannot substitute for the knowledge and practical experience that doctors and nurses have administering vaccines. Pharmacists are not as knowledgeable about diagnosing the difference between cardiac arrest, anaphylaxis and fainting and most pharmacies don’t have lifesaving defibrillators.
The limited training pharmacists get in vaccines will not be able to cover all the contraindications for the 57 different unique vaccines available24 now in the U.S. or the nearly 260 vaccines in development.25
Ensuring informed consent and accurate screening to consider family and individual medical histories will be challenging in the back of a pharmacy or a grocery store. Certain allergies, fevers, weakened immune systems, seizures, pregnancy, Guillan-Barre Syndrome and other reactions post vaccination are all reasons listed on the CDC’s Vaccine Information Statements indicating a possible reason to not vaccinate.
It is also a stretch to think pharmacists are going to report reactions to the Vaccine Adverse Events Reporting System (VAERS)26 or warn parents about the statute of limitations and instructions for filing a claim with the National Vaccine Injury Compensation Program,27 which has paid out over $4.4 billion28 to vaccine victims.
Rules Carry the Same Effect as Law
Administrative rules, while not law, carry the same effect as law. State legislatures delegate rule-making authority to the state agencies, boards of health, or health commissioners tasked with implementing state law, however, they are not supposed to change or add to what is in statute.
As more concerned citizens have made significant impact in stopping bad vaccine bills, some state health departments have turned to the rule process to add more mandates or restrict vaccine exemptions.
Additionally, there has been a trend in recent years for some state legislators who are influenced by the medical trade lobby to move the task of setting vaccine mandates or setting the criteria for vaccine exemptions completely out of the legislature and into the hands of state employees.
It is a widespread problem that many state agencies abuse their power and write rules that go beyond the scope of the state statute they are implementing. Many state’s administrative procedures acts do not give the average citizen sufficient opportunities to give feedback that will be sincerely considered.
Because state employees are not elected, state residents don’t have any recourse to remove them from their jobs as they are able to do with elected legislators who restrict or eliminate rights.
In the 2020 legislative session, NVIC Advocacy tracked and issued action alerts on proposed administrative rule changes in four states, Oklahoma, Washington, Wisconsin, and Wyoming. NVIC Advocacy team members and like-minded groups worked together in these states to stop these four rule changes.
The Oklahoma rule change would have restricted vaccine exemptions by requiring the completion of a mandatory health department educational presentation in order to obtain a religious or personal belief exemption. Strong opposition to this attempted restriction to exemptions helped ensure that the rule was amended to remove this burden on exemptions in Oklahoma.
Washington, Wisconsin and Wyoming proposed new vaccine mandates through rule. Local vaccine informed consent and health freedom groups came through in large numbers attending public comment sessions and submitting comments, engaging more families concerned about expanding vaccine schedules and communicating with legislators to ask them to oppose the rule changes as well.
This resulted in all of these proposed rule changes for new vaccine mandates being withdrawn. Proposed rule changes are typically published in state registers. It is important to watch the state health and education agency registers for proposed rules regarding vaccine requirements and exemptions.
Links to these state registers are available on the NVIC law pages. Sometimes contacting your legislators about proposed rules that force more vaccines or restrict vaccine exemptions can be helpful if the legislator contacts the agency and ask them to back off.
Legislators, especially those who sit on powerful appropriation committees setting state budgets, can have more of an influence than the average citizen. NVIC is opposed to unelected unaccountable state employees setting required vaccine schedules.
A good bill to file in states where the legislature has abdicated its power to control what vaccines are mandated on its citizens would be to repeal these laws and return control back to legislators who must face voters at the ballot box.
Comparing Recent Sessions to 2020
232 bills represent the most proposed vaccine-related bills NVIC has recorded in the history of the NVIC Advocacy Portal, surpassing the previous all-time high of 221 bills introduced in 2019. It is important to note that four states (Montana, Nevada, North Dakota and Texas) meet biennially to consider new bills and do not hold a legislative session in even years.
It is remarkable that this record number of vaccine-related bills were proposed with these four states not participating in the 2020 legislative session. The number of states proposing bills in 2020 that affected NVIC’s mission remained similar to last year: 39 and the District of Columbia compared to 40 and the District of Columbia in 2019.
There were fewer bills that NVIC opposed in 2020 compared to last year (123 versus 137). There were more bills filed that NVIC supported in 2020 than in any other session. NVIC supported 99 bills this session, which is 22 more positive bills than the previous record-breaking number of 77 bills NVIC supported in 2019.
Enlightened legislators are not only listening to concerned constituents in greater numbers, many more are continuing or beginning to resist aggressive lobbying efforts by the vaccine industry, medical trade and other groups, whose positions and profits benefit from laws that force children and adults to use every vaccine sold by pharmaceutical companies and recommended by public health officials.
Only eight bad vaccine bills passed out of the 123 that NVIC opposed in the 2020 legislative session, which was 10 less than the 18 bad vaccine bills that passed last year. Individual citizen involvement in the legislative process, through personal communications and education of legislators, continues to make a significant impact year after year on the outcomes of vaccine related bills in state legislatures.
NVIC predicts that the continued attack on vaccine exemptions and bills to expand emergency powers and mandate fast tracked COVID-19 vaccines after they are licensed and recommended by the federal government will drive even more Americans in every state to get more involved in the legislative process at every level in the years to come.
What Can You Do?
NVIC expects that the vaccine industry and their medical trade association partners will step up lobbying efforts to restrict or remove vaccine exemptions in 2021 since so many of their bills failed in 2020.
Please become a registered user of the free online NVIC Advocacy Portal and check in often to learn about ways to personally educate your legislators when vaccine bills that affect your rights are moving in your state. Please encourage your family and all of your friends to do the same.
Clearly your efforts are making a much more significant difference than the mainstream media and those pushing “no exceptions” forced vaccination policies and laws are willing to admit, and your active participation is vital to protecting informed consent rights and vaccine choices in America. If you see inaccurate information in the media, please take the time to respond by making a constructive comment online.
You can also email the journalist or call the media outlet and provide accurate, well referenced Diseases and Vaccines information and accurate state vaccine law information, which you can find on our website NVIC.org. NVIC’s illustrated and fully referenced Guide to Reforming Vaccine Policy and Law is another good vaccine education tool for legislators and friends and family, too.
The same holds true if you are censored online for providing accurate information about vaccination, infectious diseases and health. Contest it and educate those doing the censoring. The information seeds you plant today can make a difference tomorrow and into the future.
Yes, the challenges are great but so are the opportunities to educate and empower legislators and residents of every state to defend vaccine freedom of choice. NVIC is committed to continuing to make that happen and we look forward to working with you through the NVIC Advocacy Portal to help you protect vaccine informed consent rights in your state in 2021 and beyond.
from Articles https://ift.tt/32V5fbU
via IFTTT
Mexico Tackles COVID-19 Pandemic With Junk Food Bans
While most mainstream media pundits and American health authorities remain mum about the influence of nutrition and lifestyle on the risks of COVID-19 and its prognosis, more than a dozen states in Mexico have decided to combat the pandemic by banning the sale of junk food to minors.
Mexico Bans Junk Food to Curtail COVID-19 Death Toll
As reported by NPR, September 14, 2020:1
“First Oaxaca's state legislature passed a ban on selling or giving out high-calorie packaged foods and sugar-sweetened drinks to minors on Aug. 5. Less than two weeks later, Tabasco state approved a prohibition, too. Now at least a dozen other states are considering similar legislation.
‘I know it can sound a bit drastic but we had to take action now,’ says Magaly López, a lawmaker in Oaxaca's Congress who spearheaded the ban. More than 70,000 Mexicans have died from COVID-19, the world's fourth-highest recorded death toll, according to tracking by Johns Hopkins University.
Two-thirds of those who died in Mexico had an underlying medical condition such as obesity, diabetes, hypertension and cardiovascular problems, according to Health Department officials. That has led to a new urgency to change diets so that the younger generation doesn't suffer those ailments.”
Adults are also urged to cut back their consumption of junk food to curtail their risk of COVID-19 and other health issues. This includes the consumption of soda, which assistant health secretary Hugo López-Gatell has referred to as "bottled poison."2,3
Legislators are still pondering how to enforce the ban, but according to NPR, punishment for sale of junk food to minors could potentially include fines or even jail time.
López-Gatell is reportedly considering making the ban a permanent law in order to protect the health and well-being of Mexican youth moving forward. This would be no easy task, he admits, considering the powerful commercial interests at play. Critics also point out that, in all likelihood, the ban will simply shift business from grocery stores to unregulated street vendors.
Interestingly, when NPR interviewed teenagers around Mexico City and Oaxaca state, they found most “knew about health problems related to junk food” and seemed receptive to the ban. One 16-year-old girl said, “I'd be frustrated at first if I couldn't buy a Coke, but I'd adapt. And maybe I'd think twice and buy fruit or something healthy instead."
Nutrition Plays an Important Role in COVID-19 Susceptibility
As reported in “Junk Food Companies Responsible for COVID-19 Susceptibility,” underlying health conditions such as obesity, heart disease and diabetes have emerged as key factors in COVID-19 fatalities.
In one study,4,5 more than 99% of people who died from COVID-19-related complications had underlying medical conditions. Among those fatalities, 76.1% had high blood pressure, 35.5% had diabetes and 33% had heart disease.
Another study6 revealed that among 18- to 49-year-olds hospitalized due to COVID-19, obesity was the most prevalent underlying condition, just ahead of hypertension. Processed foods, junk foods and soft drinks are key culprits in the development of these chronic diseases, and therefore have a key role to play in COVID-19 hospitalizations and deaths.
London-based cardiologist Dr. Aseem Malhotra has been among those warning that poor diet can increase your risk of dying from COVID-19. He told BBC that ultraprocessed foods make up more than half the calories consumed by the British, and if you suffer from obesity, Type 2 diabetes and high blood pressure — all of which are linked to poor diet — your risk of mortality from COVID-19 increases tenfold.7
Malhotra also noted8 that eating nutritious foods for even one month could help you lose weight, put Type 2 diabetes into remission and improve your health considerably, thereby improving your chance of survival should you contract COVID-19.
Dr. Robert Lustig, Emeritus Professor of pediatrics in the division of endocrinology at the University of California, San Francisco, has also been outspoken about the connection between diet and COVID-19 risks, stating:9
"I've heard COVID-19 referred to a beast, because it doesn't distinguish. In point of fact, it doesn't distinguish who it infects. But it does distinguish who it kills.
Other than the elderly, it's those who are Black, obese, and/or have pre-existing conditions. What distinguished these three demographics? Ultra-processed food. Because ultra-processed food sets you up for inflammation, which COVID-19 is happy to exploit ... Time to rethink your menu."
Even Mild Obesity Increases Risk for COVID-19 Complications
Importantly, even mild obesity can have significant implications for COVID-19. According to Italian researchers who analyzed10 data from 482 COVID-19 patients, “Obesity is a strong, independent risk factor for respiratory failure, admission to the ICU and death among COVID-19 patients,” and the extent of risk is dependent on your level of obesity. In a press release, lead author Dr. Matteo Rottoli stated:11
"Health care practitioners should be aware that people with any grade of obesity, not just the severely obese, are a population at risk. Extra caution should be used for hospitalized COVID-19 patients with obesity, as they are likely to experience a quick deterioration towards respiratory failure, and to require intensive care admission."
Specifically, patients with mild obesity had a 2.5 times greater risk of respiratory failure and a five times greater risk of being admitted to an ICU compared to nonobese patients. Those with a BMI of 35 and over were also 12 times more likely to die from COVID-19.12
British Report Links Obesity to COVID-19 Severity and Death
Similarly, a July 2020 report13 by Public Health England described the results of two systematic reviews,14 one of which showed that excess weight worsened COVID-19 severity, and the other that obese patients were more likely to die from the disease compared to nonobese patients. Here too, the risk of hospitalization, intensive care treatment and death all progressively increased along with BMI. Compared to healthy weight patients, patients with a BMI above 25 kg/m2 were:
- 2.03 times more likely to suffer critical illness
- 6.98 times more likely to need respiratory support
- 3.68 times more likely to die
Yet another study15,16 published May 2, 2020, on the preprint server medRxiv found obesity doubles your risk of being hospitalized for COVID-19. According to the authors:17
“These findings suggest that modification of lifestyle may help to reduce the risk of COVID-19 and could be a useful adjunct to other interventions, such as social distancing and shielding of high risk.”
Pandemic Has Highlighted Role of Junk Food in Health
In an editorial18 published in the BMJ, three researchers cited the role of the food industry in driving up rates of obesity and ultimately causing more COVID-19 deaths. According to the authors, “It is now clear that the food industry shares the blame not only for the obesity pandemic but also for the severity of COVID-19 disease and its devastating consequences.”
They not only called on the food industry to stop promoting unhealthy food and drinks immediately, but also called on governments to force reformulation of junk foods to better support health.
As noted by Bill Maher in the video above, obesity has always killed us, albeit slowly. “Mixed with COVID, it kills you fast,” he says. So far, Mexico appears to be the only nation that has taken the matter seriously enough to actually implement an all-out ban on junk food for children and teens.
Other noteworthy exceptions include the town of Huntington, New York, where town officials have urged residents to “go on a diet because [with] COVID-19, you’re twice as likely to have a poor outcome if you’re obese.”
The U.K. is also targeting obesity as part of the country’s coronavirus prevention strategy by restricting junk food ads.19 July 23, 2020, Prime Minister Boris Johnson announced he intends to ban TV junk food advertising before 9 p.m. and limit in-store promotions. Online ads for unhealthy foods may also be banned.20
Studies Stress Nutrition in Fight Against COVID-19
Two additional studies are worthy of note. The first, published in the May 2020 issue of Pakistan Journal of Medical Sciences,21 points out that “Optimal nutrition and dietary nutrient intake impact the immune system, therefore the only sustainable way to survive in current context is to strengthen the immune system,” and that “A proper diet can ensure that the body is in proper state to defeat the virus.”
To optimize your chances of surviving COVID-19 and minimizing its symptoms, the authors provide both dietary guidelines and good food practices to minimize the risk of food contaminants. Included in the dietary guidelines are recommendations to:
- Eat four servings of fruit such as guava, apple, banana, strawberry, cantaloupe melon, grapefruit, pineapple, papaya, orange, Longman fruit, blackcurrant and pummelo daily
- Eat five servings of fresh vegetables daily and avoid overcooking them to prevent loss of nutrients
- Include nuts and coconut in your diet
- Include animal foods such as red meat, poultry, fish, eggs and milk
- Avoid soda and other sweetened beverages and drink pure water instead
Unfortunately, the guidelines include the recommendation to avoid healthy saturated fats such as butter, coconut oil, cheese, ghee and cream, and to use unsaturated fats only. While some unsaturated fat sources are perfectly healthy, such as avocados, fish and nuts, others really should be avoided.
Industrially processed seed oils are fats to be diligently avoided and this includes oils like soybean oil, canola oil and corn oil. The second study, published in the July 2020 issue of Brain, Behavior and Immunity, notes that:22
“The high rate of consumption of diets high in saturated fats, sugars, and refined carbohydrates (collectively called Western diet, WD) worldwide, contribute to the prevalence of obesity and type 2 diabetes, and could place these populations at an increased risk for severe COVID-19 pathology and mortality.
WD consumption activates the innate immune system and impairs adaptive immunity, leading to chronic inflammation and impaired host defense against viruses.
Furthermore, peripheral inflammation caused by COVID-19 may have long-term consequences in those that recover, leading to chronic medical conditions such as dementia and neurodegenerative disease, likely through neuroinflammatory mechanisms that can be compounded by an unhealthy diet.
Thus, now more than ever, wider access to healthy foods should be a top priority and individuals should be mindful of healthy eating habits to reduce susceptibility to and long-term complications from COVID-19.”
My Dietary Recommendations
It really did not take long before it became apparent that the COVID-19 pandemic was illustrative of a far more widespread pandemic, namely that of insulin resistance.
All of the comorbidities that dramatically increase your COVID-19 risks (including your risk of symptomatic COVID-19 illness, hospitalization and complications resulting in death) are rooted in insulin resistance. Remove the insulin resistance, along with vitamin D deficiency, and very few people — except for very old and frail individuals — would be at significant risk from SARS-CoV-2 infection.
So, it really is high time to start looking at how we can improve our health in general, and avoid insulin resistance in particular. A healthy population simply isn’t going to be as vulnerable to infectious diseases like COVID-19.
Aside from the general dietary recommendations listed above (with the exception of the recommendation to replace saturated fats with soy, canola and corn oils), I recommend:
• Adopting a cyclical ketogenic diet, which involves radically limiting carbs (replacing them with healthy fats and moderate amounts of protein) until you're close to or at your ideal weight.
This includes avoiding all ultraprocessed foods and also limiting added sugars to a maximum of 25 grams per day (15 grams a day if you're insulin resistant or diabetic). This will allow your body to start burning fat rather than carbohydrates as its primary fuel and increase the sensitivity of your insulin receptors.
Once you have regained your ideal body weight, then you can cycle carbs back in a few times a week. One of the best books written on this subject is my classic “Fat for Fuel.”
• Restricting your eating window to six to eight hours each day, making sure to eat your last meal at least three hours before bedtime. This is known as time-restricted eating or intermittent fasting, and is a powerful intervention to reduce insulin resistance and restore metabolic flexibility.
Additionally, get regular exercise each week and increase physical movement throughout your waking hours, with the goal of sitting less than three hours a day. Making sure you’re getting sufficient sleep (typically eight hours for most adults) and tending to your emotional health are also important factors that can influence your weight, general health and immune function.
from Articles https://ift.tt/3crfvM7
via IFTTT
MKRdezign
Powered by Blogger.