COVID Jabs Are Killing Two People for Every Person Saved
In the video above, Russel Brand discusses the conflicts of interest that arise when a regulatory agency is funded by the industry it is charged with regulating. Take the U.S. Food and Drug Administration, for example. In years past, the FDA was funded entirely by U.S. taxpayers.
Today, nearly 45% of its annual budget comes from user fees paid by the drug companies that seek approval for a given product, Brand says. This transition from public to corporate funding has had a significant impact on how the agency operates, and it’s clearly not in the public’s best interest.
Brand cites data showing the FDA has gone from a drug approval rate of 38% in 2005 to 61% in 2018. In situations where a drug is aimed at a disease where few medication options already exist, 89% of new drug applications are approved on the first try.
Has drug development simply gotten that much better? Probably not. The fact is that drug companies view the FDA’s user fees as payment for service rendered, and that service includes approval. They’re not paying for the FDA to turn them down.
Why FDA and Big Pharma Have a Trust Problem
In response to the COVID-19 pandemic, the FDA issued emergency use authorizations for completely novel types of “vaccine” in a matter of weeks. While some applaud this speediness, it’s worth remembering that as speedy approvals have increased with other drugs, so have the number found to be harmful after the fact.
Data cited by Brand show that 21% of FDA approved medications ultimately had to be removed from the market or be given a black box warning. Essentially, if you’re taking a newly approved drug, the chances that this drug will be found to be extremely dangerous is 1 in 5, which is hardly encouraging!
A 2017 Yale study1 found the situation is even more dire than that, showing nearly 1 in 3 FDA approved drugs ends up having new safety issues detected in the years following approval.
The FDA is also allowing drug makers to profit at the expense of public health by allowing them to “claim success in trials based on proxy measurements instead of clinical outcomes like survival rates or cures, which take more time to evaluate,” Caroline Chen notes in a June 2018 ProPublica article.2
FDA Advisers Receive Payouts to Approve Drugs
In addition to that, “pay-later conflicts of interest” are widespread, according to an investigation by the journal Science.3 This is when doctors who advise the FDA or sit on drug panels that are in charge of drug approval are paid by drug makers AFTER the approval is a done deal.
Science examined 107 physician FDA advisers who voted on drug approvals. Of those, 40 ended up receiving more than $10,000 in post hoc earnings from the drug company whose drug they voted to approve; 26 of them got more than $100,000 and six were paid more than $1 million. FDA advisers who help drug makers gain approval also reap rewards in other ways. As noted by Science:4
“The FDA says its rules, along with federal laws, stop employees from improperly cashing in on their government service. But Science found that employees at the agency often reap later rewards — jobs or consulting work — from the makers of the drugs …
A 2016 study found that 15 of the 26 employees who left the agency later worked or consulted for the biopharmaceutical industry. Of the more than $24 million in personal payments or research support from industry to the 16 top-earning advisers, 93% came from the makers of drugs those advisers previously reviewed.”
FDA Has Already Lost Most of Its Credibility
As argued by Brand, the data is rather unequivocal. It tells us corruption is rampant and the FDA has completely abandoned its charter to ensure public health and safety. It’s really just there to give the appearance that someone is looking out for public health, while in actuality it’s a venue through which drug makers are enabled to profit from unsafe and unproven drugs.
The sad reality is that while FDA approval used to mean something, today it has basically lost all meaning. Just because a drug is FDA-approved doesn’t mean it’s been proven safe and effective.
Again and again, drugs are found to have serious safety issues in the years after their approval. As a result, drug companies are allowed to benefit while public health is sacrificed, which is precisely the situation that the FDA was created to prevent.
FDA Approves COVID Boosters for Seniors
September 17, 2021, the FDA approved the Pfizer-BioNTech COVID shot Comirnaty as a third-dose booster for people over the age of 65 and other high-risk individuals. As reported by The Vaccine Reaction September 19, 2021:5
“Despite not convening the Vaccines and Related Biologic Products Advisory Committee (VRBPAC) last month to vote on effectiveness and safety of the Pfizer-BioNTech COVID-19 vaccine (licensed under the name COMIRNATY), the U.S. Food and Drug Administration (FDA) convened the advisory committee on Friday, Sept. 17, 2021 to vote on booster doses of the vaccine.
The FDA asked the VRBPAC to vote ‘yes’ or ‘no’ on the following question: Do the safety and effectiveness data from clinical trial C4591001 support approval of a COMIRNATY booster dose administered at least six months after completion of the primary series for use in individual 16 years of age and older?
The C4591001 booster dose study did not include any subjects under 18 years of age and only 12 subjects 65-85 years of age in Phase 1 of the trial and none in Phase 2/3.”
At the end of the day, 16 of the 18 VRBPAC members voted “no” on approving a Comirnaty booster dose for people over the age of 16. A second vote was then hastily thrown together, after members indicated they’d be comfortable recommending a booster for seniors and “people at high risk of severe COVID-19,” which the FDA is defining as health care workers and those at increased risk of exposure due to their occupation.
This unscheduled second vote passed unanimously. However, as reported by The Vaccine Reaction:6
“It’s important to note the data VRBPAC was asked to consider for Vote #2 is different than for Vote #1. For Vote #2 they were instructed to consider the ‘totality of scientific evidence available’ — not just Pfizer’s booster dose clinical trial.
Had the VRBPAC been required to only consider the evidence provided by Pfizer, it would have had to base its decision on data from only 12 subjects 65 years and older in Phase 1 of the trial because they were not included in Phase 2/3. The particular evidence basis for VRBPAC’s approval of a booster dose for this group was not specified.”
What’s more, the FDA suddenly shifted from “individuals at high risk of severe COVID-19” infection, to having it apply to “health care workers or others at high risk of occupational exposure.”
“This effectively shifted the focus from those who were at high risk of become severely ill from COVID-19 to those who are simply at high risk of being exposed, which will greatly expand the scope of those recommended to have a booster dose,” The Vaccine Reaction states.7
In a September 19, 2021, appearance on CBS News,8 director of the National Institutes of Health Dr. Francis Collins stated he fully expects the FDA to extend boosters beyond seniors aged 65 and older, health care workers and others at high risk of occupational exposure.
1 in 1,000 mRNA Shots Results in Heart Inflammation
So, the FDA claims the Pfizer shot is safe and effective enough to warrant a third booster for certain groups. But is it? According to a retrospective study9,10 by the University of Ottawa Heart Institute, 1 in 1,000 mRNA injections (Pfizer and Moderna) have resulted in myopericarditis, i.e., inflammation of the heart or heart sack, within one month of the shot, although symptom onset typically occurred within days.
The study was posted on the preprint server medRxiv September 16, 2021, the day before the FDA voted “yes” on boosters for the elderly and certain high-risk groups. As explained by the authors:11
“This study is a prospective collection and review of all cases with a myocarditis/pericarditis diagnosis over a 2-month period at an academic medical center … Patients were identified by admission and discharge diagnoses which included myocarditis or pericarditis. Inclusion criteria: in receipt of mRNA vaccine within one month prior to presentation …
Diagnosis was based on clinical presentation, ECG/echo findings and serial troponins and was confirmed in each case by CMR. Incidence was estimated from total doses of mRNA vaccine administered in the Ottawa region for the matching time-period. This data was obtained from the Public Health Agency of Ottawa …
Results: 32 patients were identified over the period of interest. Eighteen patients were diagnosed with myocarditis; 12 with myopericarditis; and 2 with pericarditis alone. The median age was 33 years (18-65 years). The sex ratio was 2 females to 29 males.
In 5 cases, symptoms developed after only a single dose of mRNA vaccine. In 27 patients, symptoms developed after their second dose of. Median time between vaccine dose and symptoms was 1.5 days …
Chest pain was the commonest symptom, but many others were reported. Non-syncopal non-sustained ventricular tachycardia was seen in only a single case. Median LV ejection fraction (EF) was 57% (44-66%). Nine patients had an LVEF below the normal threshold of 55%.
Incidence of myopericarditis overall was approximately 10 cases for every 10,000 inoculations. This is the largest series in the literature to clearly relate the temporal relationship between mRNA COVID vaccination, symptoms and CMR findings.”
COVID Shots May Be Killing Two for Every Life Saved
According to expert testimony given during the September 17, 2021, FDA Vaccine Advisory Committee meeting (see video above),12 the shots may in fact be killing far more people than they’re saving.
According to Dr. Joseph Fraiman, an emergency medicine physician in New Orleans, there’s no clinical evidence to prove the COVID shots are saving more people than they harm. He told the committee they ought to:
“Demand the booster trials are large enough to find a reduction in hospitalizations. Without this data we, the medical establishment, cannot confidently call out anti-COVID-vaccine activists who publicly claim the vaccines harm more than they save, especially in the young and healthy. The fact we do not have the clinical evidence to say these activists are wrong should terrify us all.”
Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, then went on to show what Fraiman feared the most, namely that the Pfizer shot kills two people for every person it saves.
“We were led to believe that the vaccines were perfectly safe, but this is simply not true. For example, there are four times as many heart attacks in the treatment group in the Pfizer 6-month trial report. That wasn’t just bad luck.
VAERS shows heart attacks happen 71 times more often following these vaccines compared to any other vaccine,” Kirsch said, adding: “If the net all-cause mortality from the vaccines is negative, then vaccines, boosters and mandates are all nonsensical.”
Here’s a screenshot from Kirsch’s slide show, showing the number of people killed by the COVID shots, compared to the number of lives saved by them.
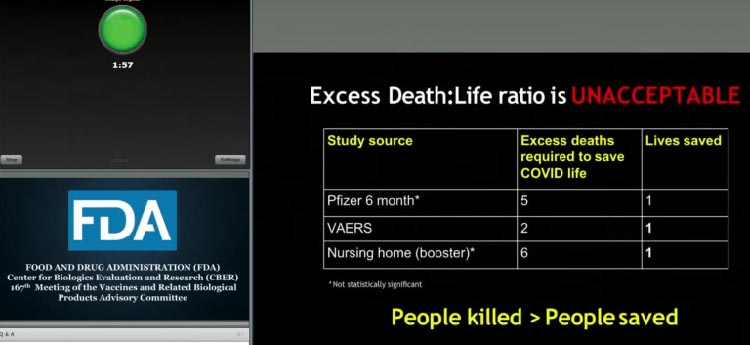
Kirsch went on to state that while the VAERS data is the only data that are statistically significant, the other two data sources are still “troubling”:
“Even if the vaccines have 100% protection, it still means we kill two people to save one life … Four experts did analyses using completely different non-U.S. data sources and all of them came up with approximately the same number of excess vaccine-related deaths — about 411 deaths per million doses.
That translates into 115,000 people who have died (due to the Covid-19 vaccines) … The real numbers confirm that we kill more than we save. And I would love everyone to look at the Israel ministry of health data on the 90+ year olds where we went from a 94.4% vaccinated group to 82.9% vaccinated in the last four months.
In the most optimistic scenario it means that 50% of the vaccinated people died and 0% of unvaccinated people died. Unless you can explain that to the American public you cannot approve the boosters.”
Kirsch also showed data suggesting 1 in 317 boys aged 16 to 17 will get myocarditis from the shots, and after a third booster, that number may reach as high as 1 in 25. He also points out that Pfizer’s Phase 3 trials must clearly be “gamed,” as “it is statistically impossible for protocol violations to be five times higher in the treatment group.” “Why has this not been investigated?” he asked.
What Do the VAERS Data Tell Us?
In a September 18, 2021, interview with The Covexit podcast, Jessica Rose, Ph.D., who holds degrees in applied mathematics, immunology, computational biology, molecular biology and biochemistry, discussed what the U.S. Vaccine Adverse Events Reporting System (VAERS) data tell us about the safety of the COVID shots.
Rose covers issues such as the magnitude of the side effects compared to other vaccination programs, the problem of under-reporting, and how causality can be assessed using the Bradford Hill Criteria. You can find a PDF of the slide show that Rose presents here.13 Here’s a summary of some of the key points made in this interview:
|
Between 2011 and 2020, the number of VAERS reports ranged between 25,408 and 49,412 for all vaccines. In 2021, with the rollout of the COVID shots, the number of VAERS reports have shot up to 521,667, as of September 3, 2021, for the COVID shots alone. |
|
Between 2011 and 2020, the total number of deaths reported to VAERS ranged between 120 and 183. In 2021, as of September 3, the reported death toll had shot up to 7,662. |
|
Cardiovascular, neurological and immunological adverse events are all being reported at rates never before seen. |
|
The estimated under-reporting factor (URF) is 31. Using this URF, the death toll from COVID shots is calculated to be 205,809 as of August 27, 2021; Bell’s palsy 81,747; herpes zoster infection 149,017; paresthesia 305,660; breakthrough COVID 365,955; myalgia 528,457; life threatening events 230,113; permanent disabilities 212,691; birth defects 7,998. |
|
If there’s no causal relationship between the shots and adverse events, we would expect side effects to occur at any given point between the vaccination date and symptom onset. This is not what we’re seeing. Death, for example, dramatically spikes within the first few days post-injection, and rapidly falls off after day 10. |
|
The Bradford Hill Criteria for causation are all satisfied. This includes but is not limited to strength of effect size, reproducibility, specificity, temporality, dose-response relationship, plausibility, coherence and reversibility. |
Children Are Now the Next Target
While the FDA voted against recommending a third booster to young adults aged 16 and over, there’s little doubt that the recommendation will soon be expanded to people under the age of 65, and eventually even young children.14 I say that because there seems to be no ceiling above which the death and disability toll is deemed too great. Why? We have not been given a straight answer, leaving us to speculate about the FDA’s intentions.
Why aren’t they concerned about safety when more than half a million side effect reports have been filed? How come nearly 15,000 reported deaths15 haven’t set off emergency alarms and in-depth investigations? As noted by Rose, 50 deaths have historically been the cutoff point at which a vaccine is pulled. We’re so far beyond that now, it seems there’s no threshold anymore.
At present, one wonders whether the FDA’s reluctance to approve a booster for younger individuals is mere show. Perhaps they’re trying to reclaim some measure of scientific authority, which was undermined by the U.S. government and Pfizer announcing the release of boosters before the FDA had even made its determination.
Whatever the case may be, I urge you to review as much data as you can before you jump on the booster bandwagon. Based on everything I’ve seen, I believe the risk of side effects is likely going to exponentially increase with each dose.
If you need a refresher on the potential mechanisms of harm, download and read Stephanie Seneff’s excellent paper,16 “Worse Than The Disease: Reviewing Some Possible Unintended Consequences of mRNA Vaccines Against COVID-19,” published in the International Journal of Vaccine Theory, Practice and Research in collaboration with Dr. Greg Nigh.
from Articles https://ift.tt/3EXIq8r
via IFTTT