There’s a medication that has been found to reduce COVID-19 mortality by 81%.1 The icing on the cake? It’s also safe, inexpensive and widely available, with decades of clinical usage suggesting it has a “high margin of safety.”2 The drug is ivermectin — a broad-spectrum anti-parasitic that also has anti-inflammatory activity.
There’s a good chance, however, that you probably haven’t heard about it. And, if you or a loved one had COVID-19, there’s also a high probability that you didn’t receive this potentially life-saving treatment, even though doctors have been begging health agencies to make it part of official COVID-19 treatment guidelines since nearly the start of the pandemic.
One professor and doctor, Hector Carvallo, who has found his science documenting ivermectin’s effectiveness for COVID-19 “quickly scrubbed from the internet," wrote to colleagues, “I am afraid we have affected the most sensitive organ on humans: the wallet.”3
In June 2021, we’re at the point when the data on ivermectin are really undebatable. It’s a safe, existing option to treat COVID-19, and an alternative to vaccination, but if it were to become mainstream, it would make the COVID-19 vaccine Emergency Use Authorization disappear because, with a readily available treatment, there’s no need for mass, emergency vaccination.
Critical Care Physicians Developed COVID Treatment Early On
Early on in the pandemic, five critical care physicians formed the Front Line COVID-19 Critical Care Working Group (FLCCC), which developed a highly effective COVID-19 treatment protocol known as MATH+.
One of those physicians, Dr. Paul Marik, a critical care doctor at Sentara Norfolk General Hospital in East Virginia, is renowned for his work in creating the “Marik Cocktail,” which significantly reduces death rates from sepsis using inexpensive, safe, generic medications.4
Not content to offer COVID-19 patients “supportive care,” which he describes as “no care at all,” he recruited some of the most knowledgeable pulmonary critical care specialists to solve the COVID-19 treatment puzzle, homing in on stopping the hyper-immune response — including multiorgan inflammation and clotting — which is what typically drives death in fatal COVID-19 cases.5
Marik told Mountain Home magazine, “As pulmonary critical care doctors we know how to treat inflammation and clotting, with corticosteroids and anticoagulants. It’s first-grade science.”6 The result was the MATH+ protocol for hospitalized COVID-19 patients mentioned earlier, which gets its name from:
Intravenous Methylprednisolone
High-dose intravenous Ascorbic acid (vitamin C)
Plus optional treatments Thiamine, zinc and vitamin D
Full dose low molecular weight Heparin
The MATH+ protocol led to high survival rates. Out of more than 100 hospitalized COVID-19 patients treated with the MATH+ protocol as of mid-April 2020, only two died. Both were in their 80s and had advanced chronic medical conditions.7
After several tweaks and updates, the prophylaxis and early outpatient treatment protocol is now known as I-MASK+8 while the hospital treatment has been renamed I-MATH+,9 due to the addition of ivermectin.
Ivermectin ‘Miracle Drug’ Silenced
In December 2020, FLCCC called for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19.10,11 In one trial, 58 volunteers took 12 milligrams of ivermectin once per month for four months.
Only four (6.96%) came down with mild COVID-19 symptoms during the May through August 2020 trial period. In comparison, 44 of 60 health care workers (73.3%) who had declined the medication were diagnosed with COVID-19.12 Mountain Home reported:13
“‘If you were to say, tell me the characteristics of a perfect drug to treat COVID-19, what would you ask for?’ he [Marik] said. ‘I think you would ask firstly for something that’s safe, that’s cheap, that’s readily available, and has anti-viral and anti-inflammatory properties.
People would say, ‘That’s ridiculous. There could not possibly be a drug that has all of those characteristics. That’s just unreasonable. But we do have such a drug. The drug is called Ivermectin.’
If it was universally distributed at a dose that costs ten American cents in India and about the cost of a Big Mac in the United States, he said, Ivermectin would save countless lives, crush variants, eliminate the need for endless big pharma booster shots, and end the pandemic all over the world.”
In June 2020, a study also found ivermectin inhibits the replication of SARS-CoV-2 in vitro, with a single treatment leading to a 5,000-fold reduction in virus after 48 hours.14 What’s more, the drug is available over-the-counter in some countries, such as France, and 3.7 billion doses have been administered in the last 40 years, with serious side effects extremely rare.15
Dr. Pierre Kory, Marik’s protégé, and a part of the group that formed FLCCC, set out to get the word out to save lives, but his calls for widespread adoption of this “miracle” drug fell on deaf ears.
Senate Committee Ignores Data on Ivermectin
December 8, 2020, Kory testified to the Senate Committee on Homeland Security and Governmental Affairs, which held a hearing on “Early Outpatient Treatment: An Essential Part of a COVID-19 Solution.” He called on the NIH, CDC and FDA to review the expansive data on ivermectin to prevent COVID-19, keep those with early symptoms from progressing and help critically ill patients recover:16,17
“‘We have a solution to this crisis,’ he said. ‘There is a drug that is proving to be of miraculous impact,’ Kory said. ‘When I say miracle, I do not use that term lightly. And I don’t want to be sensationalized when I say that.
It’s a scientific recommendation based on mountains of data that has emerged in the last three months ... from many centers and countries around the world showing the miraculous effectiveness of Ivermectin. It basically obliterates transmission of this virus. If you take it, you will not get sick.’”
Despite his impassioned pleas and astonishing science to back them up, the treatment was not only ignored by the committee but promptly eviscerated. Mountain Home reported:18
“The hearing was dead before it started … The hearing was boycotted by all seven Democrats (who have received a total of $1.3 million in big pharma bucks from Pfizer, AstraZeneca, Johnson & Johnson, Merck, Gilead, and others), and four of the seven Republicans, including Utah’s Mitt Romney (more than $3 million received from big pharma), Ohio’s Rob Portman ($542,400), and Florida’s Rick Scott (more than $1 million in stock in Gilead Sciences, maker of Remdesivir).”
Meanwhile, media reports claimed ivermectin was unproven and the World Health Organization also refused to endorse it. YouTube removed Kory’s testimony, which had nearly 9 million views, calling it a danger to the community.19 Still, the data surrounding ivermectin speaks for itself.
Ivermectin’s Impressive Data — and Legal Fights Over its Use
A scientific review by Dr. Andrew Hill at Liverpool University, funded by the WHO and UNITAID and published January 18, 2021, found ivermectin reduced COVID-19 deaths by 75%. It also increased viral clearance. This finding was based on a review of six randomized, controlled trials involving a total of 1,255 patients.20
Kory, Marik and colleagues also published their review based on 18 randomized controlled treatment trials of ivermectin in COVID-19, which found “large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.” They continued:21
“Furthermore, results from numerous controlled prophylaxis trials report significantly reduced risks of contracting COVID-19 with the regular use of ivermectin. Finally, the many examples of ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality indicate that an oral agent effective in all phases of COVID-19 has been identified.”
While an increasing number of doctors and countries have adopted ivermectin’s use for COVID-19, many more refuse it, even going so far as to prohibit its use for patients. Legal fights have ensued, with family members enlisting lawyers to battle hospital boards in order to give their dying loved ones the lifesaving pills — even when all other treatment options have been exhausted.22
‘It’s Really Almost Totalitarian’
In mid-January 2021, the NIH finally revised its guidelines on ivermectin, in large part due to the data presented by Kory and others. However, while the NIH no longer warns against its use, they also do not outright recommend it, and they did not grant ivermectin emergency use authorization. The FDA continues to warn against the use of ivermectin to treat or prevent COVID-19.23
As a result, many patients in the U.S. still struggle to access the drug, as many doctors are unwilling to prescribe it off-label against health officials’ recommendations. The reality remains that inexpensive, generic pills like ivermectin are not the ones that Big Pharma intends to become the COVID-19 savior. As Kory told Mountain Home:24
“‘Only big randomized controlled trials by big pharma/big academic medical centers are accepted by big journals, while others are rejected,’ while only studies in big journals are accepted by big public health agencies for drug recommendations, and only drugs recommended by big public health agencies ‘escape media/social media censorship.’
‘This leaves you with a system where the only thing that’s considered to have sufficient evidence or proven efficacy is essentially a big new pharmaceutical drug … If it doesn’t come from the mountaintop, it doesn’t exist … The people on the ground, we cannot do any more science that’s considered credible.
We’re discredited as controversial and as promoting unproven therapies and our Facebook groups are shut down, Twitter accounts are locked, YouTube videos are removed and demonetized. It’s really almost totalitarian what’s happening when we’re just well-meaning scientists trying to do the right thing by our patients.’”
FLCCC has published its COVID-19 treatment protocols on its website and has answers to many frequently asked questions, including how to get ivermectin.25 FLCCC remains hopeful that ivermectin will be formally adopted into national or international COVID-19 treatment guidelines in the near future.
They also receive many questions from people wondering about COVID-19 vaccines, their safety and whether or not to get vaccinated. While FLCCC does not take a position for or against them, they state, “We can only say that, for those who cannot be vaccinated, ivermectin is an equally effective measure.”26
Not only are we faced with aggressive attempts to force us into participating in a recklessly dangerous COVID-19 mass vaccination experiment, mainstream media are now drumming up concerns about the next flu season on top of it. As reported by NBC News:1
“More than a year after the pandemic started, Covid-19 is still ravaging parts of the world, but now scientists are warning that another virus could be a serious threat in the coming months: influenza.
This season, the flu virtually disappeared, with less than 2,000 lab-confirmed cases in the United States to date, according to the Centers for Disease Control and Prevention.2 In a typical flu season, the U.S. could see more than 200,000 lab-confirmed cases by this time of year, a tiny fraction of the true number of cases, estimated to range from 9 million to 45 million annually …
According to scientists like Dr. Andy Pekosz, a professor of microbiology at the Johns Hopkins Bloomberg School of Public Health, a year without much flu could lead to a year with a whole lot of flu.
‘We’ve gone over a year without a significant portion of the population getting infected with flu and getting immunity because of that,’ Pekosz said. ‘That could mean that the susceptible people in the population to flu are going to be increasing.’”
Did Masks and Social Distancing Eliminate Influenza?
According to NBC News,3 COVID-19 mitigation measures such as universal mask wearing, social distancing and lockdowns prevented transmission of influenza during the 2020/2021 season. Well, as the old saying goes, “If you believe that, I’ve got a bridge to sell you.”
First of all, the idea that masks and social distancing magically eradicated influenza, not just in the U.S. but around the world,4 is not supported by any serious science on masks, most of which actually looked at flu viruses. I’ll review some of those below.
It’s also implausible for the simple fact that COVID-19 statistics on cases, hospitalizations and mortality were all massively manipulated. There’s simply no telling how many so-called COVID-19 cases, hospitalizations and probably even deaths, were actually flu-related.
Everyone, everywhere was being tested for COVID-19. Not influenza. And anyone presenting flu-like symptoms was automatically assumed to have COVID-19. Even if the flu was tested for and was positive, any falsely positive COVID test would change the diagnosis from flu to COVID-19.
Granted, each year, one particular strain of influenza virus will tend to predominate (but will vary from region to region), but it’s never 100% just one strain. So, the likelihood of virtually all infections this past year being due to SARS-CoV-2 is ridiculously small to say the least.
Lastly, if masks and social distancing worked like magic to prevent the spread of influenza, why did these measures not eradicate SARS-CoV-2? You simply cannot have it both ways. Masking and social distancing could not possibly have prevented influenza while simultaneously having no measurable impact on COVID-19.
We’ve Long Known Masks Don’t Work Against Flu
The available research has been rather consistent: Mask wearing does not reduce the prevalence of viral upper respiratory illness, and a vast majority of these studies looked at influenza specifically. For example, a policy review paper5 published in Emerging Infectious Diseases in May 2020, which looked at 10 randomized controlled trials, found there was “no significant reduction in influenza transmission with the use of face masks.”
In 2019, a review of interventions for flu epidemics published by the World Health Organization concluded the evidence for face masks was slim, and what little benefit there was might simply be due to chance:6
“Ten relevant RCTs were identified for this review and meta-analysis to quantify the efficacy of community-based use of face masks …
In the pooled analysis, although the point estimates suggested a relative risk reduction in laboratory-confirmed influenza of 22% in the face mask group, and a reduction of 8% in the face mask group regardless of whether or not hand hygiene was also enhanced, the evidence was insufficient to exclude chance as an explanation for the reduced risk of transmission.”
Similarly, a 2020 guidance memo by the WHO pointed out that:7
“At present, there is no direct evidence … on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.”
A meta-analysis and scientific review8 led by respected researcher Thomas Jefferson, cofounder of the Cochrane Collaboration, posted on the prepublication server medRxiv in April 2020, found that, compared to no mask, mask wearing in the general population or among health care workers did not reduce influenza-like illness cases or influenza.
In one study, which looked at quarantined workers, it actually increased the risk of contracting influenza, but lowered the risk of influenza-like illness. They also found there was no difference between surgical masks and N95 respirators.
A similar finding was reported in a 2009 study,9 which compared the effectiveness of surgical masks and N95 respirators to prevent seasonal influenza in a hospital setting; 23.6% of the nurses in the surgical mask group still got the flu, as did 22.9% of those who wore N95 respirators.
Seeing how we’ve been encouraged to use cloth masks, it’s worth noting that research10 published in 2015 actually found health care workers who wore cloth masks had a 72% higher rate of lab-confirmed respiratory virus infections, compared to those wearing medical masks or controls (who used standard practices that included occasional medical mask wearing).
According to the authors, “the results caution against the use of cloth masks … Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
Mask Mandates Had No Impact on COVID-19
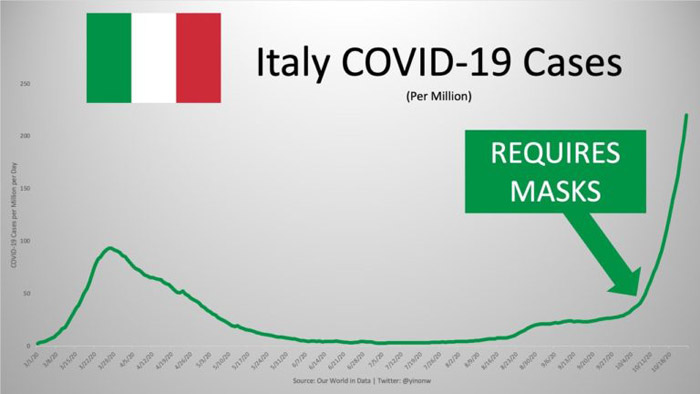
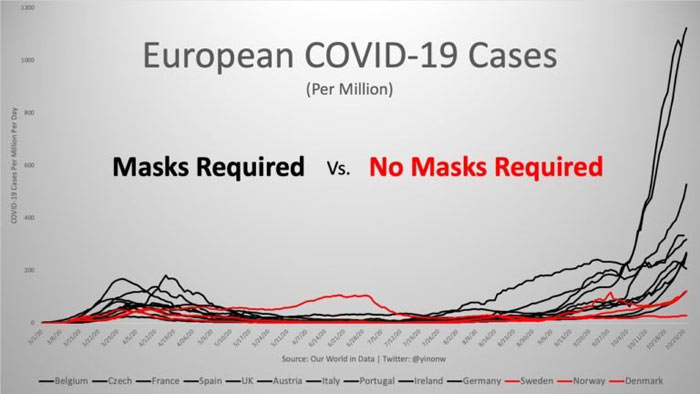
COVID-19 statistics also defy the idea that masks made any difference. In his article,11 “These 12 Graphs Show Mask Mandates Do Nothing to Stop COVID,” bioengineer Yinon Weiss points out that “No matter how strictly mask laws are enforced nor the level of mask compliance the population follows, cases all fall and rise around the same time.”
To see all of the graphs, check out Weiss’ article.12 Here are just a select few to bring home the point:
Social distancing, meanwhile, at best only led to a plateau in infectious spread, according to researchers at the University of Rochester and Cornell University,13 while lockdowns had a net negative effect.14 According to a report15 by Canadian pediatric infectious disease specialist Dr. Ari Joffe, lockdown harms are about 10 times greater than the benefits.
Coming Next: Gene-Based Combo Shots
As detailed in “How COVID Vaccines Can Cause Blood Clots and More,” the gene-based COVID-19 “vaccines” are a disaster in the making. As of May 14, 2021, the U.S. Vaccine Adverse Event Reporting System (VAERS) had logged 227,805 adverse events following COVID vaccination, including 4,201 deaths and 18,528 serious injuries.16
This included 293 injuries among 12- to -17-year-olds, 23 of which were rated serious. Of the deaths, two were under the age of 16, 23% occurred within 48 hours of vaccination and 20% were due to cardiac disorders. And remember, only 1% to 10% of adverse effects and deaths are reported to VAERS, so the real-world number of deaths could range from 42,000 to 420,000.
In a recent interview with Stephanie Seneff, Ph.D., and Judy Mikovits, Ph.D., we reviewed several of the ways in which these vaccines destroy your health. Importantly, it’s been fairly well-established that the primary damage in COVID-19 is caused by the spike protein, and this is what these vaccines are programming your body to produce.
Despite there being very obvious problems with this technology, vaccine scientists are moving full steam ahead to produce several additional gene-based vaccines, including:
• The first COVID-flu RNA vaccine17 — This combo vaccine is currently being tested on ferrets. The vaccine, made by NovaVax, combines NanoFlu, a quadrivalent seasonal flu vaccine, with an as-of-yet unapproved COVID-19 vaccine candidate called NVX-CoV2373.18 This COVID vaccine contains spike proteins produced by moth cells infected with a genetically engineered from the genetic sequence of the first strain of SARS-CoV-2.19,20
• A pneumococcal-COVID booster shot21 — This combo shot, made by Pfizer, is currently being tested on adults over 65 who have already been fully vaccinated against COVID-19. The shot combines the company’s pneumonia vaccine (pneumococcal conjugate vaccine) with a third dose of its current mRNA COVID-19 vaccine.
• mRNA seasonal influenza vaccines22 — The same mRNA technology used in Moderna’s and Pfizer’s COVID vaccines are now also being employed to develop seasonal flu vaccines. One advantage, from a production standpoint, is that such a vaccine can be developed in as little as one month. This would give researchers more time to determine which strains are in circulation that particular season.
We’re Speeding Toward Disaster
What no one is asking or talking about is what might happen if you instruct your body to continuously make spike proteins against several different types of viruses on a continuous basis, perhaps for years on end, if not the rest of your life.
No one knows just how long the cellular instructions remain viable as those studies have never been done. Even worse, they will not be keeping track of who was vaccinated and who wasn’t when people die, making it impossible to pin the blame on the vaccine.
Already, a growing list of physicians and scientists are warning that the COVID-19 shots may end up being a form of mass euthanasia. Many predict mass deaths among the vaccinated to occur within the next several years as their immune function breaks down and cardiovascular damage sets in. The idea that we’re going to add several gene therapy shots into an annual regimen will only exacerbate the predicted deaths.
Circling back to where we started, you can expect to see a new round of fear-mongering crop up as we head into fall and winter, this time badgering you to get your seasonal flu shot on top of the COVID-19 vaccine, plus a booster.
According to Moderna CEO Stephanie Bancel, those who got their first and second shots in December 2020 and January 2021 should prepare to get a third booster shot around September 2021.23 Pfizer CEO Albert Bourla has also stated that a booster may be required eight to 12 months after the initial two doses.24
Who knows, the way things are speeding along, perhaps NovaVax’s RNA-based COVID-flu combo shot will be ready for prime time by then too. I hate to be a pessimist, but I don’t foresee a happy ending to this trend. Your best bet is to take your time and don’t be so quick to offer up your body as a guinea pig for these gene-based injections. In time, the truth will become apparent, if it isn’t already.
Those with power, such as the wealthy are more likely to blame others for having shortcomings and they are also less troubled by reports of inequality, according to recent research.
from Top Health News -- ScienceDaily https://ift.tt/3gZPF4D
A new study finds that the persistence of a marker of chronic cellular stress, previously associated with neurodegenerative diseases such as amyotrophic lateral sclerosis (ALS) and frontotemporal dementia (FTD), also takes place in the brains of Huntington's disease (HD) patients.
from Top Health News -- ScienceDaily https://ift.tt/3xSmO9n
A groundbreaking study found that stem cells reduce the amount of virus causing AIDS, boost the body's antiviral immunity, and restore the gut's lymphoid follicles damaged by HIV. It provided a roadmap for multi-pronged HIV eradication strategies.
from Top Health News -- ScienceDaily https://ift.tt/3xLGFXv
A new biocompatible polymer-based composite material could soon replace metal plates in treating difficult and unstable fractures. The newly-developed material is as strong as dental composites yet non-toxic.
from Top Health News -- ScienceDaily https://ift.tt/3j8hEBV
Scientists have identified an internal communication network in mammals that may regulate tissue repair and inflammation, providing new insights on how diseases such as obesity and inflammatory skin disorders develop.
from Top Health News -- ScienceDaily https://ift.tt/3zQAlQs
Researchers were able to show for the first time that a very low calorie diet significantly alters the composition of the microbiota present in the human gut. The researchers report that dieting results in an increase of specific bacteria - notably Clostridioides difficile, which is associated with antibiotic-induced diarrhea and colitis.
from Top Health News -- ScienceDaily https://ift.tt/2TYCtFe
A typical Western high-fat diet can increase the risk of painful disorders common in people with conditions such as diabetes or obesity, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/3j3kV5v
A rare genetic defect that affects the so-called ALG2 gene can cause serious metabolic diseases in humans. Until now, its rareness and complexity made it difficult to study this congenital glycosylation disorder. A research team has finally succeeded in introducing the underlying mutation in the ALG2 gene in a fish model, allowing the causes of these complex diseases to be studied at the molecular level.
from Top Health News -- ScienceDaily https://ift.tt/2UyrlPS
Children who were exposed to higher levels of trace minerals manganese and selenium during their mothers' pregnancy had a lower risk of high blood pressure in childhood, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/3xN0vBP
Researchers have designed a deep learning-based system that accurately identifies individual skin stem cells grown under artificial conditions and tracks their motion. Using this system to perform quality control of stem cell cultures could improve the speed and efficiency of growing skin grafts for use in regenerative medicine and may also be useful for other types of stem cell cultures.
from Top Health News -- ScienceDaily https://ift.tt/3gU275Y
Pairing blueberry pie with a scoop of ice cream is a nice summer treat. Aside from being tasty, this combination might also help people take up more of the 'superfruit's' nutrients, such as anthocyanins. Researchers show that a protein found in cow's milk helped rats absorb more blueberry anthocyanins and their byproducts, boosting accessibility to these good-for-you nutrients.
from Top Health News -- ScienceDaily https://ift.tt/3gWTl7e
For patients who have inflammatory bowel syndrome (IBS), the condition is literally a pain in the gut. Chronic -- or long-term -- abdominal pain is common, and there are currently no effective treatment options for this debilitating symptom. In a new study, researchers identify a new potential source of relief: a molecule derived from spider venom. In experiments with mice, they found that one dose could stop symptoms associated with IBS pain.
from Top Health News -- ScienceDaily https://ift.tt/3gSo7Q2
A new paper describes persistent symptoms six months after acute COVID-19, even in young home isolated people. The most common symptoms were loss of smell and/or taste, fatigue, shortness of breath, impaired concentration, and memory problems.
from Top Health News -- ScienceDaily https://ift.tt/3qpCvCf
Researchers have developed an artificial intelligence-based brain age prediction model to quantify deviations from a healthy brain-aging trajectory in patients with mild cognitive impairment, according to a new study. The model has the potential to aid in early detection of cognitive impairment at an individual level.
from Top Health News -- ScienceDaily https://ift.tt/3da789k
Researchers have found that high levels of a normal protein associated with reduced heart disease also protect against Alzheimer's-like damage in mice, opening up new approaches to slowing or stopping brain damage and cognitive decline in people with Alzheimer's.
from Top Health News -- ScienceDaily https://ift.tt/3gVJH4Y
A new study in U.S.-born children from Spanish-speaking families finds that minority language exposure does not threaten the acquisition of English by children in the U.S. and that there is no trade-off between English and Spanish. Rather, children reliably acquire English by age 5, and their total language knowledge is greater to the degree that they also acquire Spanish. Children's level of English knowledge was independent of their level of Spanish knowledge.
from Top Health News -- ScienceDaily https://ift.tt/3zVpzbU
In an interview with a reporter from the Washington Examiner, Nicholas Wade, retired science writer for The New York Times, postulated the reason the media and others didn’t further explore the idea that the SARS-CoV-2 virus leaked from a lab was that the theory was initially and publicly proposed by then-President Trump.1
Wade believes the theory became politically polarized, burying the possibility it would be fully and independently explored. In April 2020, Trump made a comment that he had seen evidence supporting the theory that SARS-CoV-2 originated in a lab in China. At a White House event, he was asked about the evidence, to which he replied, “I cannot tell you that. I'm not allowed to tell you that.”2
His inability to disclose the source was immediately pounced upon by the media, prompting headlines that stated he claimed to have evidence but cited no details. Just days later, mainstream media began refuting Trump's comment, claiming the virus was not “cooked up in a Chinese lab,”3 and headlines proclaimed there was “‘Exactly Zero’ Evidence COVID-19 Came From a Lab.”4
Many reporters also claimed what one reporter in the LA Times wrote: “The story has all the earmarks of a conspiracy theory.”5 In this case, however, the truth is beginning to come out. As I’ve reported in the past months, many scientists believe the evidence demonstrates it is nearly impossible for the virus to have developed in nature.6 Within the past month the idea that the virus originated in a lab in Wuhan, China, has been gaining mainstream media attention.7
The questions appeared to start after the World Health Organization’s joint report with Beijing was released, which concluded the lab leak hypothesis was “extremely unlikely.”8 However, as demonstrated by interviews with at least one member of the investigation team, it appeared the group’s assessment at the lab was not thorough.
Challenging the idea of the origins of the virus has been seen as career suicide for scientists,9 but the recent release of emails10 from Dr. Anthony Fauci, director of the National Institute for Allergy and Infectious Diseases (NIAID) and chief medical adviser to the president, has shed new light that may ultimately create an environment where the truth will be exposed.
Fauci Works With Group to Quash Lab Leak Theory
Under the Freedom of Information Act, BuzzFeed obtained and published online11 over 3,000 pages of emails written to and from Fauci from various sources. The emails revealed an exchange between Fauci and Peter Daszak, president of EcoHealth Alliance based in New York.
In the published documents is a telling email from Daszak to Fauci, “to say a personal thank you on behalf of our staff and collaborators.”12 This email came hours after Fauci publicly dismissed the idea that SARS-CoV-2 was accidentally leaked from a Wuhan lab.
Earlier in the day the Washington Examiner13 reported that Fauci was asked directly about the hypothesis the virus leaked from a lab and he said the scientific evidence “is totally consistent with a jump of a species from an animal to a human.”
EcoHealth Alliance is a research group that secured a grant from the NIH to do research on coronaviruses in Wuhan before the pandemic broke in 2019.14 As reported in a February 2021 article in the Austin American-Statesman, the original grant from the NIH was for $3.4 million awarded in 2014 to an organization, “which aims to protect people from viruses that jump from species to species."15
EcoHealth Alliance turned around and hired the Wuhan Institute of Virology (WIV), with which they had been collaborating since 2004,16 paying $598,500 over five years.17 WIV had reportedly secured approval from the NIH and the U.S. State Department to do the research.
In February 2021, the Austin American-Statesman reporter attempted to refute the claim that Fauci and the NIH had funded gain-of-function research "on a bat coronavirus, which ‘created’ SARS-CoV-2,"18 despite incriminating evidence to the contrary as I have reported. But now, as I will show below, Fauci’s emails show that he knew much more than he was admitting to.
The very person who funded and worked closely with WIV was also appointed to the joint inspection team led by WHO and Beijing.19 The report was criticized over its strong conclusions that were based on little evidence. In a later 60 Minutes interview, Daszak admitted they had taken at face value the word of the Chinese officials in their investigation.20
NIH Finally Seeks Accountability for Millions in Grant Money
Early in 2020, the NIH pulled the multimillion-dollar grant from EcoHealth Alliance and then reinstated it in July with what Daszak termed “absurd conditions.”21 In a press release from EcoHealth Alliance they expressed displeasure at the conditions placed on the research grant, writing:22
“We were initially pleased to learn that the National Institutes of Health had reversed its indefensible decision to terminate our funding for a five year research project on emerging coronaviruses, during this coronavirus pandemic.
However, NIH's letter cynically reinstates and instantly suspends EcoHealth Alliance’s funding, then attempts to impose impossible and irrelevant conditions that will effectively block us from continuing this critical work.”
The Wall Street Journal reported some of the conditions under which EcoHealth Alliance could continue to receive funding. These included:23
A sample of the new coronavirus that Wuhan researchers used for genetic sequencing.
Arrange an inspection of the WIV by an outside team of scientists that would review the records “with specific attention to addressing the question of whether WIV staff had SARS-CoV-2 in their possession prior to December 2019."
In their response to the letter from the NIH outlining the conditions of the reinstatement, The Wall Street Journal reports, "EcoHealth Alliance said in its response that it hadn’t sent any grant funds to the Wuhan Institute before the grant was suspended, though it has provided funding to the institute in previous years."24
Daszak called the demands for information about how millions of taxpayer dollars were being spent “heinous,” and in an email to Nature, his partner scientist at WIV, Shi Zhengli, called it “outrageous.”25 Shi Zhengli is the WIV virologist who has been working with EcoHealth Alliance for over 15 years on viruses originating in bats.
In a statement to Nature, Daszak expressed concern that the additional information requested by the NIH about how millions of dollars are being spent was “pressure of a very aggressive administration.”26 Tapping into what is known to be a strong motivating factor — fear — he insinuated that the work being done by EcoHealth Alliance was all that is standing between any virus and human health, saying:27
“And it turns out that they decided that this issue and our work is going to be one of the angles of attack. That’s extremely unfortunate. The winner in all of this is the virus, and not just this virus — SARS-CoV-2 — but all the other viruses.”
Fauci Plays Word Games in Gain-of-Function Research Funding
As shared in this 15-minute video,28 Fauci has been a chief supporter of gain-of-function research. In 2014, the Obama Administration put a ban on gain-of-function research, which Fauci reversed in 2017. The research, according to the NIH guidelines, did not follow safety protocols in the specific grant to the EcoHealth Alliance shared with WIV.
That same lab was cited in 2018 for having substandard safety protocols. As noted in the video, in response to the pandemic, The Hill’s Rising, a morning news show, shared that Fauci pushed for more gain-of-function research, mentioning the Global Virome Project (GVP).29
The goal of GVP is to raise several trillion dollars to fund the discovery of zoonotic virus threats to humans,30 which includes gain-of-function research. Interestingly, the same Peter Daszak who is head of EcoHealth Alliance, receiving multimillion-dollar grants from the U.S. government, is also the secretary and treasurer of GVP.31
Daszak’s influence in suppressing information that the pandemic could have had a lab origin runs even deeper. In a Freedom of Information Act release, U.S. Right to Know32 found Daszak had penned a paper published in the Lancet that was central to the argument dismissing the idea the virus could have been released from a lab.
He orchestrated the paper signed by 27 scientists to “avoid the appearance of a political statement.”33 Getting back to Fauci’s finger in the pie, it is apparent from his answers in the video above that he now denies ever having funded gain-of-function research, even though there's irrefutable evidence that he did as I reported in, “The Biggest Flip-Flop Ever — Who's Going to Jail?”
Science Writer Makes Strong Argument for Lab Leak Origin
In an interview with a reporter from the Washington Examiner, Wade talked about what would happen if it were accepted that virologists indeed developed SARS-CoV-2 in the lab.34
"Well, this is of course one of the reasons virologists have not been too keen to explore this possibility. I think there will definitely be a public backlash. People will want to scrutinize much more closely the safety conditions virologists thought were adequate and what experiments they were doing."
Wade has been interviewed by several reporters in response to a paper he wrote titled, "Origin of COVID — Following the Clues: Did People or Nature Open Pandora's Box at Wuhan?"35 In this paper he stated that if we're ever to solve the mystery of where this novel virus came from, people must be willing to follow the science as “it offers the only sure thread through the maze.”
Unlike Fauci, who appears to be intent on distancing himself and the NIH from responsibility for the research that appears to have resulted in the virus and ultimately the financial and mental health disaster that followed, Wade presents a balanced approach to the data and goes on to write:36
"It's important to note that so far there is no direct evidence for either theory. Each depends on a set of reasonable conjectures but so far lacks proof. So I have only clues, not conclusions, to offer. But those clues point in a specific direction."
To summarize his paper, Wade believes the preponderance of clues lean toward the virus originating in a laboratory setting, most likely from the Wuhan Institute of Virology, after having undergone manipulation to increase infectiousness and pathology in humans.
In the meantime, the arguments laid out by government officials and supported in the media for the past year in support of natural origin are grounded in inconclusive speculations that require you to throw out scientifically possible scenarios. Wade writes:37
"It seems to me that proponents of lab escape can explain all the available facts about SARS2 considerably more easily than can those who favor natural emergence. It’s documented that researchers at the Wuhan Institute of Virology were doing gain-of-function experiments designed to make coronaviruses infect human cells and humanized mice.
This is exactly the kind of experiment from which a SARS2-like virus could have emerged. The researchers were not vaccinated against the viruses under study, and they were working in the minimal safety conditions of a BSL2 laboratory. So escape of a virus would not be at all surprising.”
According to the regional director of the European office of the World Health Organization, Hans Henri Kluge, a new coronavirus variant called “Delta” (its scientific name being B.1.617.2 and originating in India) is “poised to take hold” in Europe, which may necessitate renewed lockdowns.1
In a June 10, 2021, article, The Hill reported that the SARS-CoV-2 Delta variant “can spread quickly and infect those who have received one of two vaccine doses at higher rates than the fully vaccinated.”2
According to Kluge, Europe is facing the same situation as they did back in the winter of 2020, when cases rapidly rose, resulting in “a devastating resurgence, lockdowns and loss of life.” “Let’s not make that mistake again,” Kluge said during the press conference.
Indian Variant Refuels Fear
The Delta variant is now the dominant strain in the U.K., where a surge in cases, supposedly, has occurred predominantly among younger people between the ages of 12 and 20.3
Research by Public Health England (PHE) suggests two doses of Pfizer’s mRNA COVID shot is 88% effective against the Delta variant, while AstraZeneca’s DNA injection is “supposedly” 60% effective. After a single dose, either of the shots was only 33% protective against symptomatic illness.4,5
However, while single-dose recipients are said to be at greater risk than those having received two doses, more fully “vaccinated” people have actually died from this variant. According to the PHE, of the 42 Britons who had died with the Delta variant as of mid-June 2021, 12 had received two doses of gene therapy, compared to just seven single-dose recipients.6
More importantly, a June 11, 2021, PHE report7 shows that as a hospital patient, you are six times more likely to die of the COVID Delta variant if you are fully vaccinated, than if you are not vaccinated at all.
The information shows up in Table 6 of the 77-page document, which are labled as the attendance to emergency care and deaths by vaccination status and confirmed Delta cases from February 1, 2021, to June 7, 2021.
Of 33,206 Delta variant cases admitted to the hospital, 19,573 were not vaccinated. Of those, 23 (or 0.1175%) died. But, of the 13,633 patients who were vaccinated with either one or two doses, 19 (or 0.1393%) died, which is an 18.6% higher death rate than for the unvaccinated patients. Seven of the 5,393 patients who were partially vaccine with one dose died, or 0.1297%.
Of the 1,785 patients who had both vaccine doses 14 days or more before admission, 12 (or 0.6722%) died. This death rate is 5.72 times higher than that for unvaccinated patients. Put another way, if all 33,206 patients had been fully vaccinated, there would have been 223 deaths.
The PHE also claims the Delta variant is 64% more likely to transmit within households than the Kent (Alpha) variant that had previously dominated, and that it’s 40% more transmissible outdoors.8
Knowing what we now know about how science and statistics are being manipulated to give the appearance of a serious problem where there is none, I take these statements and data with a grain of salt. World leaders, however, are using the data to impose yet more restrictions. British Prime Minister Boris Johnson is now considering keeping lockdown rules in place until spring of 2022.9
Similarly, Chile, which has one of the highest COVID-jab rates in the world, with 58% of the population having received two doses and 75% having received their first dose, authorities announced a blanket lockdown across the capital of Santiago, June 10, 2021. The lockdown came in response to the highest COVID-19 case numbers since the beginning of the pandemic.10
Why Was a Disgraced Disease Modeler Relied on Yet Again?
In the U.S., Delta accounts for about 10% of cases and is doubling every two weeks, according to the former Food and Drug Administration commissioner Dr. Scott Gottlieb, who spoke about the variant on a “Face the Nation” broadcast June 13, 2021.11,12
According to Gottlieb, Delta is likely to “spike a new epidemic heading into the fall.”13 Showing just how crazy a repeat this is, Gottlieb is again citing data from Neil Ferguson. Yahoo! News calls Ferguson a “prominent British epidemiologist” but in fact, the man is beyond untrustworthy and has been thoroughly — and publicly — disgraced.
His only prominence is that of a failed statistician whose models have been repeatedly proven faulty to a ridiculous degree. The fact that Gottlieb is again using Ferguson’s models ought to set off warning bells that this is fear propaganda to justify even further COVID jabs and nothing else.
It was Ferguson’s Imperial College model14 that predicted the death of 2 million Americans and 500,000 Britons unless draconian lockdown and social distancing measures were implemented. A major flaw in his model was that he didn’t account for the fact that the susceptible population is only ever a small portion of people, never 100%.15
Ferguson was also the source of the December 2020 prediction that the Alpha variant B117 — the so-called “Kent” strain that became the predominant strain before Delta — would be 50% to 70% more contagious than previous variants circulating in the U.K., and would infect children and teens to a greater extent than previous variants.16
Well, what happened? PHE data reveal the rolling average of infections (i.e., positive tests, which may be symptomatic or asymptomatic) sharply declined starting in January 2021, from a high of 68,053 cases in early January to a low of 1,649 cases in early May 2021.17
Daily hospitalizations also dropped, as did the number of daily deaths, which plunged from a high of 1,610 in January 2021 to a low of eight on June 13, 2021.18 Apparently, the much-feared and “far more infectious” B117 strain didn’t unleash a mass-death cascade after all.
What’s more, the fact that mainstream media and health authorities have not highlighted the number of children infected or hospitalized is a clear hint that children really weren’t at great risk from B117 either. They just wanted you to fear the possibility of it being so.
In the U.S., Centers for Disease Control and Prevention data19 show adolescent hospitalizations for COVID-19 peaked at a rate of 2.1 per 100,000 hospital admissions in early January 2021. By mid-March, that had declined to 0.6 per 100,000. In April, it rose a little again, to 1.3 per 100,000. In actual numbers, we’re talking about a total of 204 teens — aged 12 to 17 — being admitted to hospital for assessment between January 2021 and March 2021.
These statistics are indeed quite far from catastrophic. Fewer than one-third required intensive care and none died. Meanwhile, there are at least four reported deaths among 12- to 17-year-olds following COVID “vaccination,” along with several hundred adverse effect reports, including dozens of cases of heart inflammation.20
As Ferguson’s calamitous predictions for Alpha variant B117 having failed to come to fruition, it appears the same fearmongering narrative has now simply shifted over to the Delta variant.
Clearly, they want us to fear for our children, as this will improve compliance with freedom-robbing measures and boost vaccine uptake. Right now, they’re having a really hard time explaining why children, whose risk of serious complications or death from COVID-19, and who aren’t a primary disease vector, would need to participate in an uncontrolled gene therapy experiment.
COVID Measures Did Not Work and Should Never Be Repeated
After a year and a half of lies and disinformation, it seems clear the technocrats pushing for a Great Reset are more than willing to make things up as they go, simply to keep the pandemic going. According to Kluge, the way out of this new phase of the pandemic is “a combination of public health measures and vaccination, not one or the other.”21
This despite the fact that we already know that none of these strategies actually work. As noted by pathologist Dr. Roger Hodkinson22 in a May 27, 2021, Last American Vagabond interview,23 masks, social distancing and lockdowns did not work and never will, and the COVID jabs are too dangerous to pursue.
In the interview above, Hodkinson reviews the very real concerns surrounding vaccine-induced spike proteins and their potentially devastating effects on health and human reproduction,24 seeing how Pfizer’s own research demonstrates free spike proteins are disseminated throughout your body within hours of injection.25,26,27
In a June 11, 2021, Daily Beast article,28 Dr. Peter Hotez — a rabid anti-vax hater — is now saying that children living in conservative “red” states, where COVID jab refusal tends to be higher, face a dangerous “nightmare summer.”
Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine, has in the past called for violent suppression of vaccine safety information, bullying parents of vaccine-injured children29 by calling them “anti-vaxxers” even though they’re discussing their children’s injuries that occurred as a result of vaccination, not because they didn’t vaccinate them.
In 2018, Hotez classified vaccine safety and pro-informed consent advocacy groups such as the National Vaccine Information Center as "hate groups" that “hate children,”30 and said we must “snuff out” (a term typically reserved for gangster style murder) the “anti-vaccine” movement.31,32 He’s also stated that vaccination “is not a choice; it’s a responsibility.”33 Not surprisingly, Hotez has very strong ties to the vaccine industry.
During a March 23, 2019, appearance on the Joe Rogan show, Hotez suggested Amazon, Facebook, Twitter, Google, Reddit, Instagram and other online platforms should hire chief scientific officers to manage, filter and regulate content.34 Hotez has also called for the use of cyberwarfare tactics against people who dare discuss potential vaccine problems, including yours truly.
No doubt, he’s loving the current Dark Age of online censorship that arose with the COVID pandemic.
“The only way to prevent these variants from gaining a foothold is to step up the pace of vaccinating everyone over the age 12 (and hopefully children younger than that by the fall),” Hotez writes in his Daily Beast article.35
“But in these robust pockets of vaccine resistance, it’s hard to imagine getting anywhere close to full coverage of young people. For example, more than 50 percent of 12- to 17-year-olds are vaccinated (received at least one dose of vaccine) in Massachusetts and Vermont, whereas less than 10 percent of those in this same age group have been vaccinated in Alabama, Louisiana, and Mississippi.
Here’s what might happen if we don’t fully vaccinate the South. First, the number of cases could accelerate in July and August, just as they did last year … In addition, we might see the new variants rise in frequency and disproportionately affect children, adolescents, and young adults, possibly including a multisystem inflammatory syndrome of children or MIS-C.
Some children’s hospitals in the region may already be seeing an acceleration in hospitalizations and ICU admissions. In fact, the CDC just reported on rising hospitalization rates among adolescents this spring.”
Hotez Overstates Risk to Children and Teens
Here, Hotez cites the CDC data36 I discussed earlier, and the way he does it ends up misrepresenting the trend. To repeat, no teenagers have died from COVID-19. And the uptick in hospitalization he’s talking about is an uptick from the mid-March low. But the April 2021 hospitalization rate for teens is still only about half the January 2021 rate (1.3 per 100,000 hospitalizations compared to 2.1 per 100,000). We are not looking at a doomsday trend here.
“The nation has to be fully and evenly vaccinated if we are to have any hope of navigating our way out of this epidemic. It’s also the surest way to protect young people in this region,” Hotez writes.37
I disagree. Already last year, in 2020, data suggested the vast majority of the global population already had full or partial natural immunity. Initially, experts estimated that 70% of the population or more would need to be exposed and develop immunity before natural herd immunity would be achieved.38
By mid-October 2020, more than a dozen scientists claimed the herd immunity threshold is actually somewhere between 43% and 9%, which means a vast majority of the global population — by then — were already at very low risk of serious illness.39,40,41,42,43 Data from Stockholm, Sweden, which didn’t shut down during 2020, showed a herd immunity threshold of 17%.44
Contrast that to the COVID jabs, which do NOT actually make you immune. You can still contract the illness and spread the virus. The vaccine makers admit the design of the shots mean they will only lessen your symptoms if or when you get infected. Theoretically, this will prevent or lower your risk of hospitalization and death.
However, on the flipside, scientists have fervently warned that the COVID shots may trigger antibody-dependent enhancement (ADE), making vaccinated individuals far more prone to serious complications and death when encountering the wild virus.
Children and teens also are not dying from COVID-19 in droves. In fact, they’re not dying from it at all, so the idea that they are in dire need of gene therapy is simply not true.
No Need to Fear Mutations
Is there cause to be concerned about the new Delta variant? Or any other variant for that matter? According to Michael Yeadon, Ph.D., a life science researcher and former vice-president and chief scientist of allergy and respiratory research at Pfizer, the answer is a firm “no.” In the interview above, which is part of the full-length documentary “Planet Lockdown,”45 Yeadon explains why.
“Basically, everything your government has told you about this virus, everything you need to do to stay safe, is a lie,” Yeadon says. “Every part of it … None of the key themes that you hear talked about — from asymptomatic transmission to top-up vaccines [i.e., booster shots] — not one of those things is supported by the science.
Every piece is cleverly chosen adjacently to something that probably is true, but is itself a lie, and has led people to where we are right now.”
When it comes to your susceptibility to variants, mutated versions of SARS-CoV-2, your resilience is not dependent on antibodies as much as it’s dependent on your T-cell immunity, also known as cellular immunity. Yeadon explains:
“You've got four or five different arms of the immune system: innate immunity, mucosal, antibody, T-cells and compliment[ary systems]. There are all of these different wonderful systems that have integrated, one with another, because it needs to defend you against all sorts of different threats in the environment.
What I'm telling you is that the emphasis on antibodies in respect of respiratory viral infections is wrong, and you can establish that quite easily by doing some searching …
I'm not saying antibodies have no role, but they're really not very important. This has been proven. There are some people in whom a natural experiment has occurred. They have a defect and they actually don't make antibodies, but they're able to fight off COVID-19, the virus SARS-CoV-2, quite well.
The way they do that is, they have T-cell immunity, cellular immunity. [T-cells] are cells that are trained to detect virus-infected cells and to kill those cells.
That's how you defend yourself against a virus. So, all of these mentions of antibody levels, it's just bunk. It is not a good measure of whether or not you're immune. It does give evidence that you've been infected, but their persistence is not important as to whether you've got immunity …
We've known this for decades. We've known about T-cells for decades. They were clearly in my undergraduate textbooks. And we've known about their importance in defending you against respiratory viruses since probably the 1970s, certainly the 1980s …
It's quite normal for RNA viruses like SARS-CoV-2, when it replicates, to make typographical errors. It’s got a very good error detection, error correction system so it doesn't make too many typos, but it does make some, and those are called ‘variants.’
It’s really important to know that if you find the variant that's most different from the sequence identified in Wuhan, that variance … is only 0.3% different from the original sequence.
I'll say it another way. If you find the most different variance, it's 99.7% identical to the original one, and I can assure you … that amount of difference is absolutely NOT possibly able to represent itself to you as a different virus. [So] when your government scientists tell you that a variant that's 0.3% different from SARS-CoV-2 could masquerade as a new virus and be a threat to your health, you should know, and I'm telling you, they are lying.”
To recap, what Yeadon is saying is that a virus cannot mutate into a version that is so dissimilar from the original that your body cannot identify it. If you have T cell immunity, your immune system will recognize the mutated virus and take care of it, just as it would with the original version of the virus.
He explains how, earlier in the pandemic, scientists obtained blood from patients who had been sickened with the SARS virus 17 or 18 years ago. SARS-CoV-1, responsible for that SARS outbreak, is only 80% similar to SARS-CoV-2. They wanted to know if the immune systems of these patients would be able to recognize SARS-CoV-2 — which they did. They still had memory T-cells against SARS-CoV-1, and those cells also recognized SARS-CoV-2, despite being only 80% similar.
Now, if a 20% difference was not enough to circumvent the immune system of these patients, why should you be concerned with a variant that is at most 0.3% different from the original SARS-CoV-2? And why would we need booster shots for these near-identical variants?
Booster Shots, a Trojan Horse?
Yeadon is extremely suspicious of the intentions behind booster shots for different variants, saying:
“You should be terrified at this point, as I am, because there's absolutely no possible justification for their manufacture. There's no possible benign interpretation of this. I believe they [the booster shots] are going to be used to damage your health and possibly kill you. Seriously. I can see no sensible interpretation other than a serious attempt at mass depopulation.
This will provide the tools to do it, and plausible deniability. They'll create another story about some sort of biological threat and you'll line up and get your top-up vaccines, and a few months or a year or so later, you'll die of some peculiar inexplicable syndrome. And they won't be able to associate it with the vaccines.
That's my belief — that they're lying to you about variants so they can make damaging top-up vaccines that you don't need at all. I think they will be used for malign purposes …”
Reject the ‘New Normal’ and Reclaim Your Life
Until or unless someone in the know steps up to the plate with a confession, we have no way of knowing whether depopulation is actually an intended outcome of these shots. Still, even if there’s no ill intent behind them, the real-world outcome may still be a mass-casualty event.
What seems clearer is that world leaders are sowing fear that is wildly disproportionate to the actual health threat of this virus and its variants, and the most logical reason for this is because they need this pandemic to continue in order to usher in the Great Reset.
The Great Reset, in turn, is part of a parallel agenda built around transhumanist ideologies, ideas and ideals, where man is merged with machine and biologically controlled through the use of nanotechnology and digital surveillance.
If I’m correct, then the COVID pandemic narrative will continue to be spun, not for the next several months but years. The fearmongering will persist until permanent tracking has been implemented, getting regular gene therapy injections have become the norm and no one does anything unless government says it’s OK. In other words, until life has been permanently turned into a hell fit for robots alone.
In the video below, talkRADIO host Julia Hartley-Brewer shares her opinion on the matter, saying that if the U.K. does not open on “Freedom Day,” June 21, 2021, as planned, then lockdowns are likely to continue forever.
She points out that the “vaccines” are working better than anyone dared hope, and a far larger portion of the population than expected have willingly taken them. People are as safe as they’re ever going to get, yet government is still vacillating, saying it’s not enough. It’s time to go back to the old normal where people are free to live their own lives, Hartley-Brewer says, and she’s absolutely right.
Boris Johnson will announce a four week delay to lockdown lifting. But Julia says: "We have to get out of this and if it's not now, it may be never. We need to get back to the old normal where we have our freedom."@JuliaHB1pic.twitter.com/slAnzM5xVx
My couch, like all of us, has had a year. It's seen a lot more of my backside than it planned to and many more meal times than should be domestically allowed.