The COVID-19 Nursing Home Massacre
The number of nursing homes has remained relatively stable since the Kaiser Family Foundation began publishing data in 2003.1 In 20182 there were 52 million people over the age of 65 and about 1.4 million who lived in nursing homes in 2019.3 In this video, the chief compliance officer of CommuniCare talks about the processes in place in their senior care facilities to combat COVID-19.
As I've shared in the past, if you want to stay healthy, it’s important that you stay away from all hospitals, except in an emergency. This pandemic has proven that the spread of infectious disease is also rampant in other types of health care facilities such as nursing homes.
Remember that people living in nursing homes or other long-term care facilities are more susceptible to infectious diseases. Mild to moderate changes in the immune system, combined with comorbidities and metabolic changes, increase susceptibility in older adults.4
Comorbid conditions can include Type 2 diabetes, renal insufficiency, cardiovascular disease and arthritis. Not each of these is directly related to an increase in susceptibility, but they can contribute to overall frailty.5 So, it comes as no surprise that nursing home residents have made up a large part of the COVID-19 deaths in the U.S. and Italy. What is surprising, is how it happened.
Italy Creates Perfect Storm in Nursing Homes
In mid-April 2020, Italy had the highest death toll in Europe from COVID-19.6 By early June they had dropped to No. 3 as recorded by the Johns Hopkins COVID-19 Resource Map, with nearly 235,000 deaths recorded in early June.7 Many occurred in the Lombardy region in Italy, their economic center.
The story likely began in early March when hospital beds were scarce and the president of Lombardy, Attilio Fontana, issued a resolution to send hospital patients with COVID-19 into nursing homes. Facilities were offered 150 euros ($163) per day for accepting these patients.8
The goal was to open hospital beds for people who were more severely ill. By late April, Italian authorities started investigating the high number of deaths of elderly residents in nursing homes. When the resolution was published, Luca Degani, president of a trade organization for 400 rest homes in the Lombardy region, was shocked. He spoke with a reporter from TRT World:9
"We read it twice, we did not want to believe what we read. The virus affects everyone indistinctly, but its lethality and gravity take a very significant logarithmic curve if people are aged and suffer multiple pathologies.
The fact that in our facilities we had people at greatest risk was a fact that had to be considered. These structures are made to let the elderly socialise and be provided with adequate care. They are not made to respond to an acute disease caused by a pandemic infection."
The deaths of nursing home residents are being called “lambs to the slaughter” and a “massacre” since health care workers were told they could not wear masks and other personal protective equipment for fear of alarming the residents.
The investigation into Pio Albergo Trivulzio, one of the largest homes in Milan, was launched when staff claimed that management downplayed the risk to them and the residents, and that they listed causes of death other than COVID-19 for those who died.10
Italian authorities have 600 other facilities under investigation and fear there are a large number of unaccounted deaths from coronavirus in nursing homes. While Fontana and the counselor for welfare are under a microscope for their actions, TRT World reports they are pointing the finger at the local Health Protection Agencies, claiming they were responsible for transferring the patients.
The chief of the Higher Health Institute in Italy believes that from early February until mid-April, more than 7,000 people died in nursing homes and that coronavirus was responsible for at least 40% of the deaths.
Experts think the actual figure may be higher since only a portion of the nursing homes were surveyed and few residents were tested.11 One health care worker from the Trivulzio described the situation to a TRT World reporter:12
"The epidemic arrived in our facility on March 13 — but we were not aware of that — when 17 patients from Sesto San Giovanni hospital (on the outskirts of Milan) were admitted with the aim of easing the pressure on hospitals that no longer had beds.
On the 17 on March we placed them in a non-Covid ward: we were not afraid because we were told by the hospital administration that they were not infected. Since then, the contagion has started spreading among doctors, nurses and health workers. In the blink of an eye, it reached, of course, the residents of the structure: the elderly."
Some States Ignore CDC Warning and the Elderly Suffer
Not every state in America has posted the same percentage of nursing home deaths. In the absence of comprehensive data, in early May The New York Times13 found that at least 28,100 residents and workers in nursing homes had died.
In the U.S., the story began March 8, 2020, when the past head of the CDC wrote to CNN that “nursing homes and other long-term care facilities are ground zero.”14 By March 18, New York Post reported the CDC told health officials, "Substantial morbidity and mortality might be averted if all long-term care facilities take steps now to prevent exposure of their residents to COVID-19.”15
Seven days later, New York Gov. Andrew Cuomo issued an order that no one should be denied admission or readmission to a long-term care facility based on a COVID-19 infection, whether confirmed or suspected. Six days after that, Gov. Phil Murphy of New Jersey issued a similar order.
The orders did not allow the nursing homes to even ask whether patients had the virus. This didn't give long-term care facilities enough information to care for their patients appropriately. While all states had the same information, Florida Gov. Ron DeSantis used a different tactic.
With the understanding that older adults are more likely to be at a higher risk, he allowed long-term care facilities to reject referrals of individuals who were infected and infectious. New York Post reported that as of mid-May, there were 5,500 deaths in nursing homes in New York state alone. This accounted for more overall deaths than any other state except New Jersey.
Nursing Home Deaths From COVID-19 Up to 80% in States
By comparison, Florida, which has a large number of long-term care homes, reported less than 750 deaths across the state, which is known for attracting retirees. In the face of these numbers, Cuomo defended his decision, and then six weeks later reversed the ruling while still insisting that the policy, which likely killed more than 5,000 people, had worked.
New York Post reported that executives from nursing homes in New York had complained that the governor should have known the mandate would kill thousands. They were unwilling to go public, however, because they feared fines and getting their licenses revoked.
The New York Times reported they identified 14 states in which more than 50% of the deaths from COVID-19 had happened in nursing homes or long-term care facilities.16
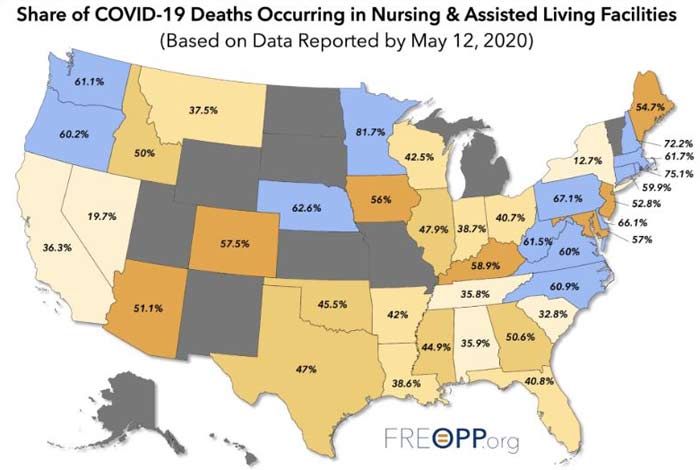
The data show that 60% of all deaths in Virginia occurred in long-term care facilities (LTCs); in Delaware, it was 66%; Rhode Island saw 75% and Minnesota attributed 81% to those in LTCs. As you can see from the map using data collected by May 12, those percentages continue to evolve.
Across the U.S., the number of deaths in nursing home residents account for 43.4% of all COVID-19 deaths.17 This is a staggering number since the 1.4 million in nursing homes account for less than 1% of the total U.S. population.
The global data remind us that we need to do a better job protecting the elderly from all infectious diseases. The BBC reports that, by far, the greatest majority of those who died in England and Wales were older than 65.
In a study from Edinburgh University, scholars argue that heavy restrictions could be lifted if greater attention were paid to shielding vulnerable populations. Professor Mark Woolhouse, an expert in infectious disease, was part of a team who evaluated data and spoke to BBC news, saying:18
"If it wasn't for the fact that it presents such a high risk of severe disease in vulnerable groups, we would never have taken the steps we have and closed down the country. If we can shield the vulnerable really well, there is no reason why we cannot lift many of the restrictions in place for others. The lockdown has come at a huge economic, social and health cost."
Rapid Spread in Hospitals Raises Number Infected
The lack of transparency in reporting illness and death from COVID-19 from nursing homes and long-term care facilities has left many shocked. As outlined in this short news report, even families are left in the dark — sometimes until after a loved one has died.
There are some clear reasons for the high number of deaths in nursing homes and other long-term care settings. Often, residents have poor overall health and weakened immune systems. They live in close quarters and receive frequent visitors and shared staff. Both visitors and staff can introduce pathogens that can spread quickly among residents.
The National Health Service (NHS) England released data reported by The Guardian suggesting that up to 20% of patients hospitalized with COVID-19 were originally infected at the hospital.19 Prime minister Boris Johnson went so far as to call the deaths from hospital-acquired COVID-19 an “epidemic.” The NHS reported that some infections were passed by hospital staff and others were passed by patients.
However, another rapid review of 40 studies in the literature indicates this number may be low. Regarding hospital-acquired infections, also called nosocomial infections, researchers noted “the incidence … can be expected to be high” since people who are potentially infected need to visit hospitals.20
The study team used major international databases to find case reports and case series with which they conducted a meta-analysis on the data. They found nosocomial infections of confirmed cases was 44% for COVID-19.
Infection Control Issues Predate COVID-19
Infection control problems in nursing homes predate the current pandemic. For instance, during the 2017-2018 flu season, the CDC estimates there were 61,000 deaths. The CDC reports the burden that year was “atypical in that it was severe for all ages.” Of the hospitalizations for flu, 67% were in adults of nursing home age, who also accounted for 83% (50,630) of all deaths.21
In a recent report by Reuters, they cited information from the U.S. Government Accountability Office showing infection prevention and control deficiencies from 2013 to 2017 in 82% of nursing homes. Of those, 48% had citations in multiple years. The deficiencies included:22
“… inadequate hand hygiene among staff, or the lack of preventative measures during disease outbreaks such as isolating sick residents and using personal protective equipment.”
Examples of actions in the nursing home included an incomplete list of those infected, lack of isolation, lack of screening for tuberculosis and allowing infected residents to continue to eat in the common dining room.
Low Vitamin D Levels Raise Risk and Mortality
May 11, 2020, Medscape.com23 released a video of Dr. JoAnn E. Manson, professor of medicine and chief of the division of preventive medicine at Harvard Medical School, in which she discussed the protective role of vitamin D against COVID-19.
She pointed to evidence suggesting that vitamin D status may play an important role in the risk of getting the infection, as well as the severity of an illness. She noted vitamin D has:24
"… an immune modulating effect and can lower inflammation, and this may be relevant to the respiratory response during COVID and the cytokine storm that's been demonstrated."
Manson is not alone in her recommendations for attaining and maintaining adequate levels of serum vitamin D to protect your health. In my article, “Are Stay-at-Home Orders Decimating Vitamin D Levels?” you’ll find further evidence relating to higher mortality rates.
As the northern hemisphere begins to experience a short reprieve over the summer months from the number of infections, it is wise to test your vitamin D levels. If COVID-19 is seasonal, a resurgence is likely come fall, which is why the time for optimizing your vitamin D level is now.
To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 nanograms per milliliter (ng/mL) and 80 ng/mL by fall. In Europe, the measurements you’re looking for are 150 nanomoles per liter (nmol/L) and 200 nmol/L.
This gives you time to take action if they are below 60 ng/mL. Your vitamin D status affects a wide range of health issues, so it’s vital to address this strategy and take control of your health. I encourage you to share this information with friends who have family members in nursing homes, people who work in long-term care facilities and even nursing homes managers.
While it’s difficult for most of us to get enough vitamin D during the winter, it’s nearly impossible for the elderly who live in nursing homes. You can have a significant impact on the health and welfare of a vulnerable population by sharing this information and taking responsible action yourself.
from Articles https://ift.tt/37BNOhf
via IFTTT