Engineers have found a way to dramatically improve the signal emitted by fluorescing nanosenors. The researchers showed they could implant sensors as deep as 5.5 centimeters in tissue and still get a strong signal. The advance allows the particles to be placed deeper within biological tissue, which could aid with cancer diagnosis or monitoring.
from Top Health News -- ScienceDaily https://ift.tt/IxvC43X
One powerful way cancer cells defend against tumor-killing immune cells is to load up their cell surface with a protein known as PD-L1. Now a team of researchers has identified a method to degrade tumor cell-surface PD-L1, thereby making tumors susceptible to immune attack.
from Top Health News -- ScienceDaily https://ift.tt/U8PjZbR
Researchers investigated genes connected to lifespan. Their research uncovered specific characteristics of these genes and revealed that two regulatory systems controlling gene expression -- circadian and pluripotency networks -- are critical to longevity. The findings have implications both in understanding how longevity evolves and in providing new targets to combat aging and age-related diseases.
from Top Health News -- ScienceDaily https://ift.tt/PLAQmFJ
Breathing difficulties are the main cause of death following opioid use. In the UK, the number of adults entering treatment for opioid use was 140,863 in 2020/211 and opioid use remains a significant cause of premature death, contributing to 3,726 drug-related deaths last year. Opioid misuse causes death by supressing respiratory activity. New research points to a novel treatment for respiratory depression associated with opioid use that administers electrical pulses to the back of the neck, helping patients regain respiratory control following high dosage opioid use. This could offer an alternative to pharmacological treatments, which can cause withdrawal symptoms, heart problems and can negatively affect the central nervous system.
from Top Health News -- ScienceDaily https://ift.tt/7U8D3JM
Scientists have identified a new role for a protein complex at the center of a human genetic disorder called Bardet-Biedl syndrome, or BBS, for which there is currently no cure.
from Top Health News -- ScienceDaily https://ift.tt/rC9gcdm
The U.S. Food and Drug Administration amended its emergency use authorization for the Pfizer-BioNTech COVID-19 shot to allow a booster dose for children ages 5 to 11.1 The FDA’s “evaluation of safety” for the booster dose in young children was based on a study of only about 400 children, and no meeting was held with the Vaccines and Related Biological Products Advisory Committee.
The booster shot is intended to be given at least five months after the primary two-dose series has been completed, but less than one-third — only 28.8% — of U.S. children in this age group have received the first two doses of this experimental gene therapy.2
“[G]iven that these children have the lowest coronavirus vaccination rate of all eligible Americans, [as most parents have wisely avoided giving their child the jab,] public health experts are not expecting a rush for the booster,” The New York Times reported,3 and this is good news, since multiple red flags have risen regarding the use of these shots, particularly among children.
COVID Shots’ Dismal Effectiveness Wanes Rapidly
Booster shots are typically released because the initial shots aren’t working as planned. This is certainly the case with COVID-19 shots, which have been found to have dismally low effectiveness rates of 12%, according to research conducted by the New York State Department of Health.4 In their rationale for why a booster dose is now needed for children, Dr. Peter Marks, Ph.D., director of the FDA’s Center for Biologics Evaluation and Research, said:5
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations.”
From December 13, 2021, to January 24, 2022, the New York State Department of Health researchers analyzed outcomes among 852,384 children aged 12 to 17 years, and 365,502 children aged 5 to 11 years, who had received two doses of the shots. Effectiveness declined rapidly among 5- to 11-year-olds, falling from 68% to just 12%.
Protection against hospitalization also dropped, from 100% to 48%. Among 11-year-olds alone, vaccine effectiveness plunged to 11%.6 The lackluster response was blamed on the dosage discrepancies among the age groups, as 5- to 11-year-olds receive two 10-microgram Pfizer shots, while 12- to 17-year-olds receive 30-microgram shots.7
A CDC study also found that the effectiveness of two doses of Pfizer’s COVID-19 shots against symptomatic COVID-19 infection “was modest and decreased rapidly” from December 2021 to February 2022.8 The study found that two to four weeks after the second dose of Pfizer’s COVID-19 shots, effectiveness was 60.1% among 5- to 11-year-olds. This fell to just 28.9% by month 2.
A similar trend was seen among adolescents aged 12 to 15 years. Vaccine effectiveness two to four weeks after the second dose of the shots was 59.5%, and this fell to 16.6% during month two.9 Among adolescents who received a booster dose, effectiveness went back up to 71.1% two to 6.5 weeks later, but it’s not revealed what happened after that.
If data from adults are any indication, the boost in effectiveness from the booster will also be short-lived. Among adults, within four to five months post-booster, protection against emergency department and urgent care visits due to COVID-19 decreased to 66%, then fell to just 31% after five months or more post-booster.10
Children’s Booster Trial Didn’t Test Effectiveness
The FDA’s decision to allow a booster dose for children was based on an ongoing Pfizer trial — the same one that it used to authorize the first set of COVID-19 shots in the 5- to 11-year-old age group.
Antibody responses were evaluated in only 67 subjects who received a booster shot seven to nine months after the two-dose primary series of shots. “The antibody level against the SARS-CoV-2 virus one month after the booster dose was increased compared to before the booster dose,” the FDA noted.11
However, there is still no data on whether the booster is effective against COVID-19, and whether the effectiveness will quickly wane, as it has with all previous shots. The New York Times also reported:12
“In the Pfizer-BioNTech clinical trial, children showed a sixfold increase in antibody levels against the original version of the virus one month after receiving the booster, compared with one month after receiving a second dose …
Laboratory tests of blood samples from a tiny subgroup of 30 children also showed 36 times the level of neutralizing antibodies against the Omicron variant compared with levels after only two doses. The study did not show how long the antibodies last or test effectiveness against Covid-19.”
High, Artificially Elevated Antibodies Come at a Cost
What’s more, the notion that increasing antibodies equates to disease protection and better health is misguided. Artificially inflated antibodies signal to your body that you’re always infected, and the resulting immune response could prove to be detrimental to your health.
Your adaptive immune system, specifically, generates antibodies that are used to fight pathogens that your body has previously encountered.13 During normal infections, your cellular immune system produces high fever and temporary T-cell elevations, along with elevated antibodies to the infection, gradually dissipate.
Ali Ellebedy, Ph.D., an associate professor of pathology & immunology at Washington University School of Medicine in St. Louis, explained, “It’s normal for antibody levels to go down after acute infection, but they don’t go down to zero; they plateau.”14 This is a normal response and isn’t a measure of waning immunity.
On the contrary, repeatedly, artificially inflating antibodies with booster shots comes with a cost and can lead to a “death zone,” accelerating the development of autoimmune conditions such as Parkinson’s, Kawasaki disease and multiple sclerosis, according to tech leader and COVID analyst Marc Girardot, who urges a retreat from the vaccination “death zone” before it’s too late.15
It’s known, for instance, that certain autoimmune diseases are seen alongside high levels of antibodies.16 Further, COVID-19 shots train your body to produce singular antibodies for one spike protein and cannot compare to the protection provided by natural immunity, which occurs after recovery from an illness. Speaking with Daniel Horowitz, pathologist Dr. Ryan Cole explained that natural infection produces broad immunity that can’t be matched by vaccination:17
"A natural infection induces hundreds upon hundreds of antibodies against all proteins of the virus, including the envelope, the membrane, the nucleocapsid, and the spike. Dozens upon dozens of these antibodies neutralize the virus when encountered again.
Additionally, because of the immune system exposure to these numerous proteins (epitomes), our T cells mount a robust memory, as well. Our T cells are the 'marines' of the immune system and the first line of defense against pathogens. T cell memory to those infected with SARSCOV1 is at 17 years and running still."
Dr. Robert Malone, the inventor of the mRNA vaccine core platform technology,18 also stated, “When it comes to COVID, public health officials have consistently downplayed and ignored natural immunity among children. Yet 81 research studies19 confirm that natural immunity to COVID is equal or superior to any ‘vaccine immunity.’”20
COVID Shots Cause Liver Failure, Other Serious Adverse Effects
A concerning number of case reports describe the development of immune-mediated and autoimmune hepatitis in the days and weeks following COVID-19 injections.21 A team of researchers collected date from such cases from 18 countries, identifying 87 patients with a median age of 48 years who developed autoimmune hepatitis-like liver injury after a COVID-19 shot.22
Typically, the liver injury was diagnosed 15 days after the shot. Most cases (59%) were attributed to Pfizer’s COVID-19 shot while 23% were linked to the Oxford-AstraZeneca shot and 18% to Moderna’s shot. All of the patients in the study recovered from the liver injury after treatment — except for one. That man developed liver failure and had to have a liver transplant. The researchers concluded:23
“SARS-CoV-2 vaccination can be associated with liver injury. Corticosteroid therapy may be beneficial in those with immune-mediated features or severe hepatitis. Outcome was generally favorable, but vaccine associated liver injury led to fulminant liver failure in one patient.”
Young children are also developing severe hepatitis at an unusually high rate and nobody knows why.24 It’s unclear how many of the children have received COVID-19 shots, but researchers did suggest that mild or asymptomatic COVID-19 infection could have left behind spike protein that’s acting as a “superantigen”25 and triggering the immune system to over-react to other viruses, such as adenovirus-41F, which is causing liver damage.26
If that’s the case, the spike protein that circulates in the body after COVID-19 shots could also be problematic, especially since “mRNA vaccines promote sustained synthesis of the SARS-CoV-2 spike protein.”27 Other concerning adverse events have also been reported.
One study published in Scientific Reports, for instance, revealed that calls to Israel’s National Emergency Medical Services (EMS) for cardiac arrest and acute coronary syndrome increased more than 25% among 16- to 39-year-olds from January to May 2021, compared to the same time period in 2019 and 2020.28
COVID-19 Case Rates Higher in Injected Children
Children are at an extremely low risk of serious illness from COVID-19, making the recommendations for COVID-19 shots, and now boosters, among this population highly questionable — even ludicrous.
“Research shows that there is no benefit to children receiving a COVID shot, and in fact, the shots can cause potential harm, adverse effects and death. According to Pfizer’s own study trial data, the chance of death in children from the shot is 107 times higher than death from COVID,” Malone stated.29
The CDC’s own data also show that COVID-19 case rates among children who have received two COVID-19 shots have been higher than rates in children who did not get the shots since February 2022.30
“That’s the first time CDC recorded a higher case rate among fully vaccinated young children since data was first collected in December 2021,” Malone said,31 and perhaps it’s harbinger of things to come. Adding a booster dose to the already dangerous, ineffective and flawed COVID-19 shot recommendations for children will only add more fuel to the fire.
This article was previously published March 22, 2019, and has been updated with new information.
A process known as "succession" occurs when one plant species replaces another.1 As explained in the National Geographic short film featured above, when an area is left to its own devices, it will naturally turn into a forest over time, replete with a wide variety of plant species, and this diversification occurs unaided by man.
The film features a man-made "forest garden" designed to mimic this kind of naturally occurring ecosystem, where fruit and nut trees grow intermingled with shrubs, herbs, vines and a variety of perennial vegetables in a seemingly wild-grown setting. According to National Geographic:2
"U.K.-based Martin Crawford is one of the pioneers of forest gardening. Starting out with a flat field in 1994, his land has been transformed into a woodland and serves as an educational resource for others interested in forest gardening.
This short film by Thomas Regnault focuses on Crawford's forest garden, which is abundant, diverse, edible and might be one answer to the future of food systems."
Diversity Allows the Entire System to Thrive
In his unconventional garden, Crawford grows 500 different edible plants and trees, yet the garden only requires a few hours of maintenance per month. This low maintenance requirement is a direct result of creating a self-sustainable and renewable ecosystem where everything is working in a symbiotic and supportive fashion.
While many today think of food production as the process of planting an annual crop, this really isn't natural, Crawford says. In a natural ecosystem, there are several layers of plant growth, starting with tall trees at the top, with shorter trees, medium and low shrubs, root crops, climbing plants and low-lying ground cover underneath.
What's more, while many of these produce edible foods directly, other plants, referred to by Crawford as "system plants," are there simply to help the system as a whole thrive. In this group you have nitrogen-fixing plants, mineral accumulators and plants that attract pollinators and insects that serve as natural pest control by eating other more harmful bugs.
Aside from being low-maintenance, this kind of diversification also protects your crops from all manner of bad weather, be it storms, excessive rains or droughts. While some may fail, others may benefit and do better, but in many cases, a majority of your crops will survive and do well no matter what the weather is doing, Crawford says.
This cannot be said for monocrop farming, where if conditions are poor, the entire crop will fail all at once. As such, having a diverse garden is key to food security. "It gives you maximum resilience," Crawford says.
How to Use Regenerative Farming Principles in Your Own Garden
Over the years, I've interviewed several pioneers in regenerative agriculture, among them, Gabe Brown, who has a regenerative farm in Bismarck, North Dakota. As explained by Brown, to grow healthy food you have to create healthy soil.
There are five basic principles to building a healthy soil ecosystem, and most of these can be implemented even if all you have is a small garden plot in your backyard:
Avoid disturbing the soil microbiome with tillage, herbicides, pesticides and fungicides — The less mechanical disturbance, the better. The same applies in your home garden.
The more you till, the faster the soil degrades and is destroyed, as it destroys soil aggregates and mycorrhizal fungi, which houses the microorganisms needed for nutrient transfer. Similarly, by adding synthetic nitrogen to the soil, the biology is radically altered — it starts consuming carbon in the soil aggregate, which destroys the soil structure.
Without soil structure water cannot infiltrate and move throughout the soil profile and be stored via organic matter. The soil aggregates also provide the home for soil biology, which is critical to producing nutrient dense food.
Protect the soil's surface with cover crops and cover crop residue — Forest and prairie land is completely covered with vegetation and this is the environment farmers need to emulate. That vegetation protects the soil not only from wind and water erosion, but also from excessive heating and cooling. These living plants are what end up actually "growing" topsoil.
In your home garden, you can use mulch, wood chips or lawn clippings to do this. You never want to leave soil bare, as bare soil will have a negative effect on soil biology and the water cycle. Cover crops and other forms of "soil armor," such as wood chips, effectively prevent water evaporation and lowers the soil temperature.
There is easily a 20-degree F difference or more between soil that is bare and soil that is covered. When air temperatures reach 90 degrees or so, soil temperatures will rise well above 100 degrees, which will dry everything out and fry the plants' roots.
"If you have good armor or residue on the soil surface, the temperature there can be in the 80-degree range. Those plants are growing. It's a huge difference in production for the producer," Brown says.
Diversify — Having a diverse array of plant life is essential, and cover crops fulfill this requirement as well. Home gardens will also benefit from cover crops, helping to improve the soil, attract beneficial insects and capture more sunlight (energy).
Maintain living roots in the ground as long as possible — In conventional farming, once a cash crop is harvested, there's nothing left in the field to capture sunlight and keep growing. Maintaining some kind of growth at all times is key. If you have a small vegetable garden, don't leave it bare once you've harvested your veggies. Instead, plant a cover crop in anticipation for the next season.
To make the transition back from cover crop to your chosen vegetables the following season, avoid the temptation to till the cover crop into the soil. Instead, use one of the following methods to kill off the cover crop and prepare the plot for new crop growth:
Stomp the cover crop into the ground with your feet or a board (simply attach two rope handles to a 2x4 board and then use the board to step down the crop)
If the cover crop has started to form seed heads, you can kill it off by rolling a crop roller or small barrel over it
Cut the growth down and leave the residue on top (although it works better if it's rolled or stepped down)
Once the cover crop has been killed off, you're ready to plant your vegetable seeds. For a small garden, use a hoe to part the cover crop remains over to the side. Create a small slice in the soil, drop in your seeds and cover with a small amount of soil. If you're planting a transplant, simply move the cover crop aside, dig the hole and plant as normal.
Integrate livestock and other animals, including insects — Centuries ago, large herds of bison and elk moved across the landscape, foraging, depositing manure and trampling vegetation into the ground. All of this is part of the natural cycle that is missing when animals are kept in concentrated animal feeding operations.
Many have started raising chickens in their backyards again and chickens are an excellent addition to a sustainable garden. Rabbits, pigeons and ducks are other alternatives that could work in some suburban areas, but even if circumstances or local laws prevent you from adding animals, be sure to plant flowering plants that attract pollinators and predator insects, as these will naturally help ward off pests that might otherwise decimate your main crop.
Tips to Help You Design Your Own Permaculture Garden
While Crawford refers to his garden as a "forest garden," it's essentially a form of permaculture garden. Permaculture epitomizes sustainability by harnessing mutually beneficial relationships to create synergistic, self-supporting ecosystems. Its principles incorporate the best of organic, biodynamic and regenerative agriculture. According to the Permaculture Institute:3
"Permaculture is an ecological design system for sustainability in all aspects of human endeavor. It teaches us how to design natural homes and abundant food production systems, regenerate degraded landscapes and ecosystems, develop ethical economies and communities and much more."
In short, permaculture is an agricultural system in which the parts of the system are all interconnected, working with nature as opposed to against it. The word "permaculture" derives from "permanent agriculture" or "permanent culture." The focus is not on any one element of the system but on the relationships among them — animals, plants, insects, microorganisms, water, soil and habitat — and how to use these relationships to create self-supporting ecosystems.
If you want to shoot for a forest garden like Crawford's, take his advice and just start planting some larger trees (or incorporate ones you already have on your property), then add smaller trees, shrubs and plants as you go along. You don't have to have it all planned out before you begin.
While there's no set formula for designing a permaculture garden, here are a few basic guidelines to consider:4,5
Copy a forest blueprint with a tree canopy that gives way to smaller trees, flanked by shrubs, with smaller shade plants under the canopy
Group plants by compatible roots and canopy systems, and by soil type, such as acid lovers in one area and drought-resistant in another
Identify microclimates in your yard and use them to your advantage, such as cooler shady corners, full sun, rocky areas and areas that receive abundant drainage
Incorporate as much diversity as possible, focusing on native plants and animals
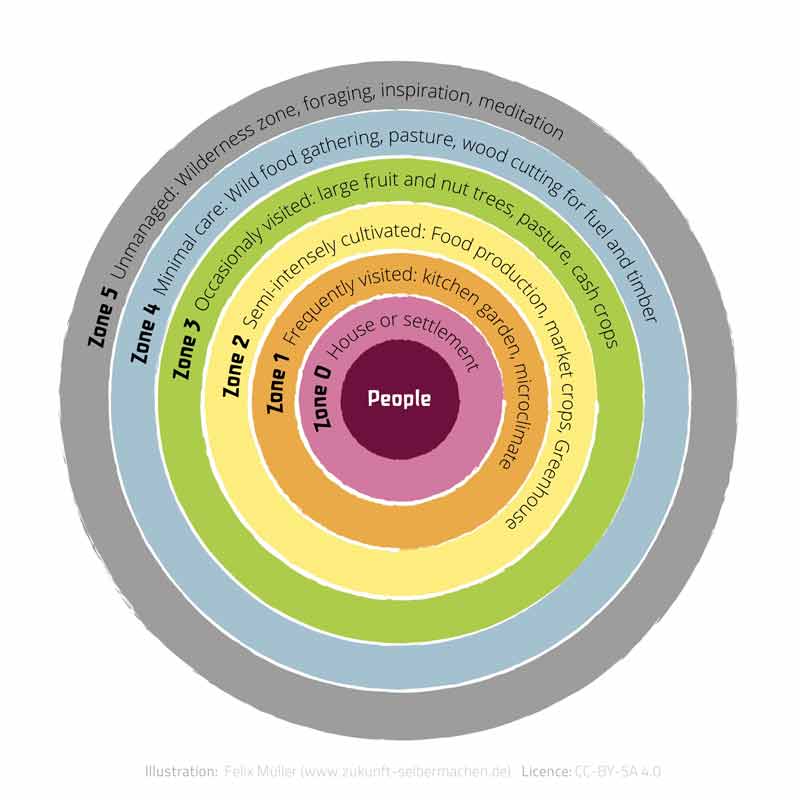
Plan your area in zones based on use and accessibility; for example, plant your herb garden and greens in the areas easiest to access, such as along the driveway or along a path near your deck
Should you have a large enough piece of land, you could go a step further and take into account the five permaculture zones as illustrated in the following diagram. At its center are you and your house, but its outermost zone is untamed wilderness.
Zones are organized in a way that maximizes energy efficiency, so activities are sorted by frequency of use, tending, visits and so on. For more detailed information about these zones, check out the Permaculture Research Institute's "Permaculture Zones Primer."6
Of the innovations that make our hearts sing, period undies have to be right up there. Virtually leak-proof and very low-maintenance, they’re a perfect alternative.
Maverick was first used as a baby name after a television show called 'Maverick' aired in the 1950s, but its popularity rose meteorically in 1986 with the release of the movie 'Top Gun.' Today, it is even used for baby girls.
from Top Health News -- ScienceDaily https://ift.tt/QlTIro6
Researchers have developed an ultrasound-guided cancer immunotherapy platform that generates systemic antitumor immunity and improves the therapeutic efficacy of immune checkpoint blockade.
from Top Health News -- ScienceDaily https://ift.tt/DcVs8GX
Another name for overprescribing medications is polypharmacy. The issue is snowballing as Big Pharma continues to develop prescription medications in the hope of lengthening life expectancy without addressing the underlying issues of the chronic diseases that affect the population. Polypharmacy may be thought of as the use of multiple medications at the same time by one person.
While the term is commonly used, there is not a single definition for polypharmacy.1 The term appears to have been in use for over 100 years according to one article that states it “was used over one and a half centuries ago to refer to issues related to multiple-drug consumption and excessive use of drugs.”2 According to a systematic review and BMC Geriatrics:3
“The most commonly reported definition of polypharmacy was the numerical definition of five or more medications daily, with definitions ranging from two or more to 11 or more medicines.”
While there has been no consensus on the number of medications, it is commonly accepted that polypharmacy is the prescription of too many medications. The concurrent use of multiple prescriptions is almost always to treat several chronic conditions at the same time. Yet, this causes side effects, can trigger additional health concerns and even cause death.
The Elderly Are Most at Risk
Polypharmacy is most common in older adults who have several risk factors and chronic health conditions that can lead to overprescription. According to the Centers for Disease Control and Prevention,4 6 in every 10 adults in the U.S. has at least one chronic health condition and 4 in 10 have two or more.
According to the National Council on Aging,5 80% of adults over 65 have at least one chronic health condition and 68% have two or more. The 10 most common are:
High blood pressure
58%
High cholesterol
47%
Arthritis
31%
Coronary heart disease
29%
Diabetes
27%
Chronic kidney disease
18%
Heart failure
14%
Depression
14%
Alzheimer's disease and dementia
11%
Chronic obstructive pulmonary disease (COPD)
11%
Physicians have multiple tools at their disposal to evaluate whether their patients are overprescribed medications, including the Beers, START (screening tool to alert to right treatment), STOPP (screening tool of older people's prescriptions), and the Medication Appropriateness Index.6
One of the most significant risk factors associated with polypharmacy is the increased potential for patients to experience adverse drug events, including death. One paper reported that “outpatients taking five or more medications had an 88% increased risk of experiencing an ADE compared to those who were taking fewer medications.”7 Nursing home residents taking nine or more medications were twice as likely to have an adverse drug event.
According to the National Institute on Aging,8 the risk of polypharmacy rises in patients who have two or more chronic conditions, and adults aged 65 and over are on more prescription medications than other age groups. One report from the CDC9 in 2019 found that 22.4% of adults aged 40 to 79 in the U.S. used at least five prescription drugs. The most common types were lipid-lowering drugs, ACE inhibitors and antidepressants.
Another health tracking poll in 201910 reported that 51% of 30- to 49-year-olds and 38% of 18- to 29-year-olds were taking prescription drugs. The number of adults taking multiple drugs increased radically as the survey participants aged. In adults 65 and older, 54% reported taking four or more drugs each day as compared to 13% in adults aged 30 to 49.
HCP Live reported on Dr. Aubrey Knight’s presentation before the 2010 AAFP Scientific Assembly, in which he cautioned the audience that until proven otherwise, any symptom in the elderly could be a drug side effect, “a medication is a poison with a desirable side effect” and advised that physicians “consider medication as a possible problem, and not just as the solution.”11
Polypharmacy Isn’t the Only Type of Overprescription
A study published in The BMJ in 201312 found “In utero exposure to both SSRIs and nonselective monoamine reuptake inhibitors (tricyclic antidepressants) was associated with an increased risk of autism spectrum disorders, particularly without intellectual disability” in the offspring.
In 2014, The New York Times reported13 that data presented by the CDC showed that 10,000 toddlers aged 2 or 3 years old were being medicated for attention deficit hyperactivity disorder. These medications were given outside established guidelines for the pediatric population. The report also showed that toddlers at greatest risk were covered by Medicaid.
While these numbers are significant, they are dwarfed by data released in 2014 from the Citizens Commission on Human Rights,14 which showed hundreds of thousands of toddlers were prescribed psychiatric drugs and more than 274,000 children from birth to 1 year old were included in that mix. According to their figures the numbers of children aged birth to 1 year old on these medications were:15
249,669 on antianxiety drugs (such as Xanax, Klonopin and Ativan)
26,406 on antidepressants (such as Prozac, Zoloft and Paxil)
1,422 on ADHD drugs (such as Ritalin, Adderall and Concerta)
654 on antipsychotics (such as Risperdal, Seroquel, and Zyprexa)
In the 2- to 3-year-old age group, the commission found 318,997 were on antianxiety drugs, 46,102 on antidepressants and 3,760 on antipsychotics. These shocking figures challenge logic. How and why are so many children and even babies, on addictive and dangerous mind-altering medications? This surely is overprescribing even in the strictest sense!
Even though the prescription rates had slightly declined by 2017,16 a new problem had popped up, with doctors prescribing antipsychotics to children for off-label purposes not specifically approved by the FDA. Then, with the rates of adult17 and childhood18 mental disorders rising dramatically during the pandemic, the prescriptions for psychiatric drugs in children began to rise again — and this time at a polypharmacy level.
A study published in the Nordic Journal of Psychiatry in March 202219 noted that not only was the use of antipsychotics in children increasing, but that polypharmacy — prescribing of multiple psychotic drugs — to children is now occurring. Researchers said:
“… polypharmacy occurred in 44.9% of the new antipsychotic users, being more frequent in girls (55.5%) than in boys (44.5%). The two most frequent concomitant psychotropic drug classes were antidepressants (66.2%) and psychostimulants/atomoxetine (30.8%). Adolescents aged 13–15 and 16–17 years, and girls showed an increased risk of polypharmacy during antipsychotic treatment.
The use of psychostimulants/atomoxetine or antidepressants prior to initiation of antipsychotic treatment was strongly associated with polypharmacy during antipsychotic treatment.”
The study authors added that this is a “worrisome trend” and that prescribers need to “carefully evaluate the efficacy of psychotropic polypharmacy in children and adolescents.” I agree.
Even Over-the-Counter Medications Have Consequences
Over-the-counter (OTC) drugs are those you can buy at the store without a prescription. You'll find hundreds of cold preparations, antacids, pain medications and allergy relief drugs that can sometimes cause unpleasant adverse events. Common side effects can include nausea, dizziness, fatigue and bleeding in the digestive tract.
You can have drug interactions with OTC medications in the same way as with prescribed medications. OTC medications can also interact with your prescription medications or your food.
Thus, as you’re considering the number of prescription medications you are taking, don’t forget to consider the OTC drugs that you routinely use. One of the hidden dangers of polypharmacy is the chemical interactions that occur in the body when medications are mixed.
Another problem is the number of times one drug is prescribed to take care of the side effects of another. This has become known as a “prescribing cascade.”20 Consider whether you or a loved one is using OTC drugs to counteract the side effects of prescription medications.
How Can You Tell if You Are Taking Too Many Medications?
According to the Commonwealth Fund,21 people in the U.S. spend more per capita on prescription drugs than in other high-income countries.
While this article focuses on cost rather than number of prescriptions, cost alone would be one reason to reevaluate what drugs you’re taking and why. That way you’re not only potentially saving some money if you eliminate one or more drugs, but you’re checking to see if you’re overmedicated. Consider the following signs that may show you are overprescribed medication.22
You consistently visit multiple doctors — As more medical records are being kept electronically, you might think that doctors’ offices communicate with each other about your case. However, that doesn't happen.
If you see a gastroenterologist for stomach issues and a rheumatologist for your arthritis, one doctor does not know what the other doctor has prescribed. You may end up seeing your primary care physician to take care of the side effects or the drug interactions from prescriptions you received from the other two specialists — and end up on still another prescription to lessen the side effects of the others.
A new health condition develops — If you’ve been overprescribed medication, you may start developing new health conditions and symptoms. These may be a result of drug interactions or adverse drug events that go unrecognized.
They can include physical or mental symptoms such as fatigue, general aches and pains, problems with balance and motor skills and unexpected weight gain or weight loss. You may notice confusion or impaired memory, concentration problems, delayed decision-making or an inability to think rationally.
You are in a high-risk group for overprescription — People who have a higher risk of overprescription of medications include those with multiple chronic health conditions, people over age 65 and women. According to the Canadian Deprescribing Network, women are at higher risk because they have a longer life expectancy, and their physiology increases the risk of adverse drug events.23
You have access to good health care — Interestingly, people with good insurance are at higher risk for polypharmacy. It's not uncommon for people in this position to see multiple doctors who are unaware of the medications being prescribed.
You have trouble keeping up with your medication — When you're taking too many prescribed drugs, it can be difficult to remember the dosing schedule and keep up with the frequency and timing. This could be a signal that you're on too many medications and should review your current list with your primary care physician.
Financial pressure — Prescription drugs can be expensive. A potential sign that you might be taking more medication than is necessary is the added financial strain on your budget.
Take Control of Your Drug Cabinet
You can take several easy steps to help reduce the number of medications you or a loved one is taking, thus reducing the potential of an adverse drug event.
• Make a list of medications — It's helpful to begin with a list of the medications and OTC drugs you are consistently taking. This is a good starting point for yourself and to review with your primary care provider who may not know all the medication you've been prescribed by other specialists.24
It's a good idea to do this with your primary care physician at least once a year. This medication review is also important after being discharged from the hospital or rehab facility, since it's not uncommon to have been prescribed more medications while you are an inpatient.
Consider creating a chart of your medications to use during your medication review with your primary care provider. The chart can have a list of the drugs you're taking, the reason you're taking them, who prescribed them, when they were started and side effects you may be experiencing. This helps your physician see the big picture quickly without asking multiple questions that can quickly eat up your appointment time.
This also helps you to get to know your medications, why you’re taking them and how they might be affecting you. Before taking any OTC medications, talk with your pharmacist about drug interactions between the OTC and any supplement or prescribed medication you might be taking.
Bring the list with you to each of your appointments with different specialists.25 This keeps all your health care providers up to date with your treatments, nutritional supplements, prescription drugs and over-the-counter medications.
• Use one pharmacy for all prescribed medications — This allows the pharmacist to quickly ascertain whether there are any drug interactions between your prescribed medications from different doctors and answer your questions about OTC drugs and supplements.
• Pay special attention each time a new medication is prescribed — Read the label and check online resources. If you find information that is concerning, talk with your pharmacist and your doctor. There may be a different medication that can be used, or you may be able to use other strategies to address your health problem.
The bottom line is that you may not need all the medications you've been prescribed to manage your health conditions. Overprescribing sets up older adults for a downward spiral of increasing side effects and worsening health. A holistic approach is needed to address the key tenets of good health and create real wellness instead of attempting to cover up symptoms with more pills.
As just one example, in a study26 of older depressed adults, 80% experienced a significant reduction in symptoms after taking strength training for 10 weeks. This caused the researchers to conclude that exercise was “an effective antidepressant in depressed elders, while also improving strength, morale and quality of life.”27
There is no magic pill that fixes symptoms, removes illness and restores vigor. However, there are lifestyle choices you can make that go a long way toward achieving your goals.
Consider starting with strategies that move you toward better health, including getting an adequate amount of quality sleep, incorporating intermittent fasting, making low-carbohydrate food choices and incorporating high-quality fats from organically and sustainably grown meat and dairy.
This article was previously published February 23, 2019, and has been updated with new information.
The use of sewage sludge as fertilizer for your food, renamed "biosolids" by slick industry PR firms, is a growing and under-publicized threat to human health. Sewage sludge is the residue generated during the treatment of domestic waste and contains a cocktail of hazardous substances from industry, hospitals and humans — anything that is discharged into the sewage system.
Some city sewer lines run right to the factories, allowing them to dump their waste into the city's sewage treatment plants. This saves industries a lot of money because once a regulated chemical or waste enters the sewer line, they're suddenly exempt from EPA regulation.
While many, including myself, have highlighted the serious dangers posed by wide application of sewage sludge for decades, new awareness was created by a report from the U.S. Inspector General's office (OIG) titled, "EPA Unable to Assess the Impact of Hundreds of Unregulated Pollutants in Land-Applied Biosolids on Human Health and the Environment."
Beware the Biosolid Scam
A video (posted above), "Biosludged," from Health Ranger/Natural News, added more concerns to the already recognized biosolid threats of heavy metals, drugs, hormones and antibiotic resistance, namely bioterrorism. Anyone could introduce deadly substances into the sewage system, such as the Ebola virus, which would, courtesy of wide biosolids application, be disseminated to harm a large amount of people.
What people put down their toilet comes "right back on their dinner plate a few weeks later," warns the video, citing the discovery of the blood thinner Warfarin, the toxic herbicide and endocrine disrupter atrazine, pesticides, fungicides, pharmaceuticals, recreational drugs, industrial drugs, chemical solvents, plasticizers and disinfectants in biosolids.
"If you wouldn't put it in your garden, don't flush it down toilet," says Mike Adams, known as the Health Ranger, who adds that biosolids are the greatest environmental crime in America that most people have never heard of. While there is a Clean Water Act and Clean Air Act, a Clean Soil Act is sorely needed says Adams.
Adams and his website are admittedly controversial, but it's indisputable that the application of massive amounts of biosolids containing nitrogen and phosphorus, combined with other nitrogen-rich fertilizers, have contributed to the growing algae blooms along U.S. coasts.
This environmental destruction harms human and animal life as well as water quality. Unfortunately, many of the southern states experience greater use of biosolids as they accept excrement exported from other cities.
Serious Questions About EPA Regulation of Biosolids
In November 2018, the U.S. Inspector General's office released a scathing indictment of how the EPA regulates — or more accurately, doesn't regulate — the biosolids industry. The OIG charged that:1
"The controls over the land application of sewage sludge (biosolids), including laws, regulations, guidance, policies or activities, were incomplete or had weaknesses and may not fully protect human health and the environment.
The EPA consistently monitored biosolids for nine regulated pollutants. However, the agency lacked the data or risk assessment tools needed to make a determination on the safety of 352 pollutants found in biosolids. The EPA identified these pollutants in a variety of studies from 1989 through 2015.
Our analysis determined that the 352 pollutants include 61 designated as acutely hazardous, hazardous or priority pollutants in other programs. The Clean Water Act requires the EPA to review biosolids regulations at least every two years to identify additional pollutants and promulgate regulations for such pollutants."
What are some of the harmful pollutants the Inspector General found in biosolids?
"Unregulated pollutants identified include pharmaceuticals (e.g., ciprofloxacin, diphenhydramine and triclocarban); steroids and hormones (e.g., campesterol, cholestanol and coprostanol); and flame retardants.
The agency also identified perfluoroalkyl substances (PFASs) and perfluorooctanoate (PFOA) in biosolids research … 32 are hazardous wastes under RCRA (four of which are acutely hazardous). 35 are EPA priority pollutants. 16 are NIOSH [National Institute for Occupational Safety and Health] hazardous drugs."
Scientific Research Confirms the Dangers
Faced with the IOG's 60-page paper detailing the dangers of biosolids, the EPA had few defenses beyond, "Hazard alone does not indicate risk," and "Not all 352 pollutants found in biosolids lack data to evaluate risk. Those pollutants with sufficient data will be evaluated for risk" in the future. Is anyone relieved?
Scientific papers clearly confirm the dangers of biosolids from their persistence in the soil to their ability to enter the very crops you eat. Triclocarban, an antibiotic similar to triclosan (found in toothpaste and other consumer products) "remained years after biosolid application" says research in Environmental Science and Pollution Research.2
The antibiotics amoxicillin, ampicillin, erythromycin, oxytetracycline, sulfadimethoxine and others were detected "in sewage sludges after nearly a decade in frozen storage," says research in Science of the Total Environment.3
Perfluoroalkyl substances (PFASs), man-made chemicals the EPA admits have "adverse human health effects"4 and flame retardants (HFRs and PBDEs) were detected in spinach, tomatoes and corn from biosolid-treated soil, according to research in Science Direct.5 Pharmaceuticals were believed to enter radish tissues according to Water Research,6 and lettuce readily absorbed estrogens, according to a study published in Environmental Science and Pollution Research.7
Antibiotic Resistance Is Also a Risk From Biosolids
It should surprise no one who reads my newsletter that using sewer sludge to grow food increases the already pressing problem of antibiotic resistance. The over-prescription of antibiotics to humans and livestock has created superbugs that kill thousands each year. The combination of human waste — which contains both antibiotics, pathogens and antibiotic-resistant pathogens — with hospital and industrial waste only worsens the deadly problem.
The accumulation of a metabolite of the antibiotic sulfamethoxazole "in the solid phase is less bioavailable and is hard to be desorbed in the existence of microbial activities … and may lead to the development of antibiotic-resistant bacteria and genes after discharge into the environment," warn researchers in Environmental Science and Pollution Research.8
"Ampicillin-resistant bacteria increased in [biosolid] amended soils four months after amendment and remained at least one log 10 higher 24 months later," says research in Science of the Total Environment. 9
The ubiquity of antibiotic use in medical, veterinary and agricultural practices "has instigated great environmental concern due to the toxicological effects associated with these compounds," says research in Environmental Monitoring and Assessment.10
"Some of the effects of antibiotics include development of antibiotic-resistant bacteria, making it difficult to treat diseases, variation in natural microbial communities, and enzyme activities especially in aerobic and low and intermediate anaerobic plots due to small rates of decay."
Strong Economic Forces Are Behind Biosolids
How did the deceptive term "biosolid" replace the more accurate term toxic sewer sludge? It was coined by the Water Environment Federation, says PR Watch.11
"The Water Environment Federation (WEF), the sewage sludge industry trade group that invented the Orwellian PR euphemism 'biosolids' for toxic sludge in 1991, is now 'rebranding' sewage treatment plants as 'water resource recovery facilities.'
The PR spin conveniently glosses over the toxic sewage sludge removed from the water and then heated and dumped on land for crops and grazing as 'fertilizer' or misleadingly called 'compost.' The toxins in sludge can then bioaccumulate in the meat and dairy we eat and be taken up by the food plants that feed us."
Sludge is big business and waste giant Synagro leads the industry. According to its website:12
"[Synagro] provide[s] solutions for all aspects of biosolids and residuals management needs, from land permitting and soil analysis by our nationwide technical services team to facilities development by our in-house engineering staff. Synagro provides a comprehensive scope of customer-focused solutions."
Selling sludge as "fertilizer" is the least expensive way for municipalities to get rid of their biosolids and make room for more, says In These Times.13 Corporations that sign contracts with municipalities to remove and haul the sludge are also fans of the lucrative status quo, as are farmers who appreciate inexpensive "fertilizer." But some communities are resisting.
We Don't Want Your Poop, Say Community Activists
At a hearing held in November 2018 by the Pennsylvania State Council of Farm Organizations, Darree Sicher, founder of the United Sludge Free Alliance, said one of her main concerns is that biosolids are contaminated with pharmaceuticals and flame retardants, which could lead to birth defects in livestock.14 Much of Europe incinerates rather than spreads such waste, said others at the hearing.
In January 2019, Florida state Rep. Erin Grall, R-Vero Beach, introduced a bill that would allow landowners to keep spreading imported biosolids if the landowner "can affirmatively demonstrate that the nutrients in the biosolids will not add to nutrient loadings in the watershed," which was greeted by citizen resistance.15
Residents in Washington state have similarly spoken out.16 "There's a saying that the biosolids flow downhill — I live downhill," said James Brigham, who lives near the proposed biosolids site. Delivery of the biosolids would involve 50 trucks, it was revealed at the meeting.
In April 2022 Maine became the first state to ban agricultural use of sludge to prevent further contamination from PFAS.17 In Michigan, officials established standards for applying biosolids such as sewage sludge in 2021, and in 2022 they began shutting down dairy and beef farms when PFAS were found in the water, ground and feed.18
Gardeners Beware
Toxic sewer sludge is not just an agricultural risk, "Biosludged" points out. Biosolids are also sold as lawn and garden fertilizer to homeowners despite their dangerous components.
Both Dillo Dirt and Milorganite present themselves as eco-friendly and environmentally-sound soil treatments, yet both carry warnings of serious risks to human health in their fine print. Dillo Dirt contains toxic sludge from Austin, and Milorganite is made with toxic sludge from Milwaukee, says Mike Adams. Both should be avoided at all costs.
Unfortunately, companies do not have to disclose when biosolids are used in their compost or potting soil. Composted products can even have the USDA organic label on them, and still be loaded with toxic biosolids. Milorganite is just one example.
If you grow vegetables in your garden and want to avoid toxins contained in biosolids, your best bet is to buy organic potting soil and/or compost from a local nursery you know and trust that can guarantee no biosolids have been added.
As predicted, just as hysteria about COVID-19 is winding down, another “pandemic” is poised to take its place. This time, it’s monkeypox, an infection that just so happens to mimic many of the symptoms of COVID jab-induced shingles — so much so, the Department of Health in Queensland, Australia, used the same photo to illustrate both infections (the photos have since been removed or updated1).
The first European case of monkeypox was confirmed May 7, 2022, in the U.K.2 Then, seemingly overnight, cases were being reported across the world.3 May 20, 2022, the World Health Organization held an emergency meeting to discuss reports of more than 100 suspected or confirmed cases in at least nine countries, including Belgium, France, Germany, Italy, the Netherlands, Portugal, Spain, Sweden, the U.K., the U.S., Canada and Australia.4
By the time this article goes to print, the number of countries affected and the case load totals are likely going to be significantly higher. The first case in the U.S. was reported May 18, 2022.5
By May 23, suspected monkeypox cases were reported in three additional states: New York, Florida and Utah.6 All of the patients were said to be in good condition and state health departments were in agreement that the cases posed no serious risk to the public.
President Joe Biden has stated that strict quarantine protocols are not likely to be implemented in the U.S. He has, however, already placed a $119 million order for a monkeypox vaccine.7,8
Belgium, meanwhile, has introduced a 21-day quarantine for anyone who tests positive, and the U.K. is urging anyone who has had direct contact with a confirmed case to voluntarily isolate for 21 days.9
As noted by Jimmy Dore in the video above, the worldwide monkeypox outbreak seems perfectly timed to pressure countries to relinquish health care authority to the WHO.
The World Health Assembly was voting on amendments to the International Health Regulations (IHR)10 as the first cases were being identified. I discussed the implications of these amendments in a recent article. As noted by Dore, a pandemic rehearsal conducted just last year also featured monkeypox specifically. I’ll review that further below.
What Is Monkeypox?
Monkeypox, a relative of the smallpox virus, is a typically mild viral illness, characterized by fever, headache, muscle aches, exhaustion, swollen lymph nodes and a bumpy rash that tends to start on the face before spreading to other parts of the body.
The pus-filled lesions are known as “pox.” The lesions eventually scab over and fall off after three to four weeks. The infection is not readily transmissible, as it requires direct contact with bodily fluids.
While there’s no known effective treatment, most patients recover without any treatment whatsoever. Historically, the infection has primarily plagued the African continent, where a few thousand cases are reported each year. However, many of the current cases are not linked to travel, making the outbreak in so many different areas a rare oddity. As noted by Nature magazine:11
“On 19 May, researchers in Portugal uploaded the first draft genome12 of the monkeypox virus that was detected there, but Gustavo Palacios, a virologist at the Icahn School of Medicine at Mount Sinai in New York City, emphasizes that it’s still a very early draft, and more work needs to be done before any definitive conclusions can be drawn.
What researchers can tell from this preliminary genetic data is that the strain of the monkeypox virus found in Portugal is related to a viral strain predominantly found in West Africa. This strain causes milder disease and has a lower death rate — about 1% in poor rural populations — compared with the one that circulates in Central Africa.
But exactly how much the strain causing the current outbreaks differs from the one in West Africa — and whether the cases popping up in various countries are linked to one another — remains unknown.”
Outbreaks Blamed on Gay Sex
Several of the Spanish cases were linked to a “superspreader event at an adult sauna” in Madrid, at least three Belgian cases were linked to a gay fetish festival in Antwerp,13 and cases in Italy and Tenerife have been linked to a gay pride festival on the Canary Islands.14 Health officials also claim a “notable proportion” of British cases are in the gay and bisexual community.15,16
Is the singling out of gays another ploy in the totalitarian takeover plan? Totalitarian regimes always need an enemy onto which the fear and irrational aggression of the hypnotized masses can be directed, and since the hatred against those refusing the COVID jab has significantly abated, they clearly need a new scapegoat.
It would not surprise me if, after two years of promoting the gay and trans community, the far Left will now begin to incite anger and fear against it. Why? Because it causes confusion and uncertainty. People who once showed allegiance with this group will now be splintered against them. At the end of the day, it’s all about psychological splintering and pitting various groups against each other.
It appears the monkeypox outbreak is also being used to promote The Great Reset in other ways. Already, U.K. health officials are warning the monkeypox virus may spread through consumption of infected meat,17 and we already know that eliminating meat consumption is part of the globalist agenda.
Monkeypox Simulation in 2021
Making the monkeypox outbreaks all the more suspicious is the fact that a tabletop simulation exercise of a monkeypox outbreak took place in March 2021,18 and the start date of this fictional scenario was mid-May 2022. Coincidence?
In the video above, AmazingPolly reviews the details of this simulation. She also reminds us how Event 201 ended up “predicting” the COVID pandemic to a tee, and shows how we’re now seeing a replay of “coincidences” between the monkeypox simulation and real-world events.
The monkeypox exercise was held by the Nuclear Threat Initiative (NTI), which is funded by Bill Gates. NTI was founded to assess and reduce threats associated with the proliferation of nuclear weapons,19 but they’ve since expanded to include biological threats.20 Gates has not only funded NTI pandemic simulations but has also given grants to the NTI for vaccine development in relation to biological threats.21
The final report22,23 from this event was funded by the Open Philanthropy project, which in turn is funded by Facebook cofounder Dustin Moscowitz. As reported by The Defender:24
“This ‘fictional exercise scenario’ involved the simulation of ‘a deadly, global pandemic involving an unusual strain of monkeypox virus that first emerged in the fictional nation of Brinia and spread globally over 18 months’ ...
The outcome of this ‘exercise scenario’ found the fictional pandemic, ‘caused by a terrorist attack using a pathogen engineered in a laboratory with inadequate biosafety and biosecurity provisions and weak oversight,’ led to ‘more than three billion cases and 270 million fatalities worldwide.’
The fictional start date of the monkeypox pandemic in this exercise was May 15, 2022. The first European case of monkeypox was identified on May 7, 2022.”
As mentioned, the first European case of monkeypox was in fact confirmed May 7, 2022, in the U.K.25 Not only is the date identical to that in this supposedly fictional scenario, but the country of emergence, “Brinia,” even sounds very much like “Britannica,” or “Great Britain.” Coincidence?
Key Recommendations From the Pandemic Exercise
As reported by The Defender, among the key recommendations from this monkeypox simulation were recommendations that clearly support the WHO’s takeover of pandemic preparedness and response, and the implementation of Gates’ "Global Epidemic Response & Mobilization" (GERM26) Team:27
Bolstering international systems “for pandemic risk assessment, warning, and investigating outbreak origins,” calling upon the WHO to “establish a graded, transparent, international public health alert system” and the United Nations system to “establish a new mechanism for investigating high-consequence biological events of unknown origin.”
The development and implementation of “national-level triggers for early, proactive pandemic response,” including the adaptation of the “no-regrets” approach to responding to pandemics via “anticipatory action” based on “triggers” that would automatically generate a response to “high-consequence biological events.”
The establishment of “an international entity dedicated to reducing emerging biological risks associated with rapid technology advances,” that would “support interventions throughout the bioscience and biotechnology research and development life cycle — from funding, through execution, and on to publication or commercialization.”
Anticipatory action based on triggers include everything we’ve saw during the COVID pandemic, such as mask mandates, the banning of mass gatherings, travel health screening and vaccine passports. This despite overwhelming evidence showing these strategies are ineffective at best, while being devastating to public health and economies.
Why Does Fiction so Often Turn Into Reality?
As noted by The Defender,28 Michael P. Sanger29 and Tim Hinchliffe,30 among others, fictional tabletop exercises have had an uncanny ability to predict details of near-future events. Event 201 accurately “predicted” the COVID pandemic and its focus on censorship and lockdowns.
In June 2001, Operation Dark Winter examined “the national security, intergovernmental, and information challenges of a biological attack on the American homeland,” and less than three months later, the 9/11 attacks and subsequent anthrax scare occurred. In January 2005, Operation Atlantic Storm involved the fictional scenario of a transatlantic bioterrorist attack and that same month we had the bird flu pandemic. The Defender continues:31
“Predictions for the future don’t end there, however. For instance, in September 2017, NTI and the WEF organized a roundtable discussion on the current state of biological risks presented by technology advancement in light of the Fourth Industrial Revolution.
And in January 2020, NTI and the WEF again joined forces, issuing a report titled ‘Biosecurity Innovation and Risk Reduction: A Global Framework for Accessible, Safe and Secure DNA Synthesis.’ According to the report:
‘Rapid advancements in commercially available DNA synthesis technologies — used for example to artificially create gene sequences for clinical diagnosis and treatment — pose growing risks, with the potential to cause a catastrophic biological security threat if accidentally or deliberately misused.’
Merck, whose head of corporate affairs participated in the monkeypox simulation, was the subject of an FBI and CDC investigation in November 2021 regarding 15 suspicious vials labeled “smallpox” at a Merck facility in Philadelphia.”
In a National Pulse exclusive,32 Natalie Winters also summarizes research by the Wuhan Institute of Virology (WIV), in which they “assembled monkeypox strains using methods flagged for creating ‘contagious pathogens.’”
“Are we here because of China’s experiments again?” she asks, referring to the apparent monkeypox outbreaks. The research paper33 in question was published at the end of February 2022, just a few months before the first cases suddenly appeared outside of Africa.
What Do We Know About the Monkeypox Vaccine?
The monkeypox vaccine currently being stockpiled by the U.S. and Europe is not specific for the monkeypox. It’s actually a smallpox vaccine, claimed to be 85% effective at stopping monkeypox. In the U.K., close contacts of those infected with monkeypox have reportedly already been given the smallpox vaccine — a strategy known as “ring vaccination.”34 In the U.S., there are currently two smallpox vaccines available:
• ACAM2000 was approved by the U.S. Food and Drug Administration in 2007 and has primarily been restricted to use in military personnel due to its safety risks, which include infection with the vaccine strain, vaccine shedding and death.
Package insert warnings include myocarditis and pericarditis at a rate of 5.7 per 1,000 vaccinated, encephalitis, severe skin infection, blindness, fetal death and more. Household contacts face the same risks as the vaccinated individual due to shedding.
• Jynneos (known as Imvamune in Canada or Imvanex in Europe35) was approved by the FDA in 2019. It’s an attenuated live vaccine, indicated for the prevention of smallpox and monkeypox in adults aged 18 and older, and those who cannot be vaccinated with ACAM2000 due to contraindications such as atopic dermatitis, immunocompromising conditions, breastfeeding or pregnancy. It’s the only FDA-approved monkeypox vaccine for non-military use.
The U.S. Biomedical Advanced Research and Development Authority (BARDA) has also signed a contract with Bavarian Nordic for a freeze-dried version of the Jynneos smallpox vaccine, which will give it longer shelf-life.36 Moderna already has a monkeypox vaccine in pre-clinical trials.37 It’s unclear when those trials began.
As noted by independent journalist Whitney Webb, Emergent BioSolutions and SIGA Technologies — both of which have been struggling recently — will be cashing in on the monkeypox scare:38
“Regardless of how the monkeypox situation plays out, two companies are already cashing in. As concern over monkeypox has risen, so too have the shares of Emergent BioSolutions and SIGA Technologies.
Both companies essentially have monopolies in the U.S. market, and other markets as well, on smallpox vaccines and treatments. Their main smallpox-focused products are, conveniently, also used to protect against or treat monkeypox as well. As a result, the shares of Emergent BioSolutions climbed 12% on Thursday, while those of SIGA soared 17.1%.
For these companies, the monkeypox fears are a godsend, specifically for SIGA, which produces a smallpox treatment, known by its brand name TPOXX. It is SIGA’s only product.
While some outlets have noted that the rise in the valuation of SIGA Technologies has coincided with recent concerns about monkeypox, essentially no attention has been given to the fact that the company is apparently the only piece of a powerful billionaire’s empire that isn’t currently crumbling.
That billionaire, ‘corporate raider’ Ron Perelman, has deep and controversial ties to the Clinton family and the Democratic party as well as troubling ties to Jeffery Epstein. Aside from his controlling stake in SIGA, Perelman has recently made headlines for rapidly liquidating many of his assets in a desperate bid for cash.
Similarly, Emergent BioSolutions has also been in hot water. The company, which has troubling ties to the 2001 Anthrax attacks, came under fire just under two weeks ago for engaging in a ‘cover-up’ over quality control issues relating to their production of COVID-19 vaccines.
A Congressional investigation found that quality control concerns at an Emergent-run facility led to more than 400 million doses of COVID-19 vaccines being discarded.
The Emergent factory in question had been shut down by the U.S. Food and Drug Administration (FDA) in April 2021. They were allowed to reopen last August before the government terminated the contract.”
What’s the Truth of the Matter?
In addition to Webb’s article above, which dissects the sordid histories of Emergent and SIGA, another early analysis of the new monkeypox scare that is well worth reading is Dr. Robert Malone’s Substack article,39 “Monkey Pox — Truth Versus Fearporn.” In it, he reviews what monkeypox actually is, where it came from, how it’s related to smallpox, it’s signs and symptoms, how disease spread is effectively controlled and much more.
Key take-home’s are that monkeypox is not a particularly deadly disease and one that can be readily controlled without reverting back to COVID restrictions. To quote Malone:40
“So, is the biothreat real? Is it imminent? Does it justify the global media hype? As I was waiting in an airport lounge to travel from USA to the UK two days ago, I saw a newsreel from CNN which was breathlessly reporting on this ‘threat’ while displaying historic images of patients suffering from Smallpox disease.
This provides a classical example of public health fearporn, in my opinion, and CNN should be reprimanded for broadcasting irresponsible propaganda — misinformation and disinformation — under the guise of journalism.
In my opinion, based on currently available information, Monkeypox is a virus and disease which is endemic in Africa, emerges sporadically after transmission into humans from animal hosts, and is typically spread by close human contact. It is readily controlled by classical public health measures.
It does not have a high mortality rate. Unless there has been some genetic alteration, either through evolution or intentional genetic manipulation, it is not a significant biothreat, and has never been considered a high threat pathogen in the past. So, stop the fear mongering, misinformation and disinformation.”
The way it looks right now, it appears the monkeypox outbreaks are intended to rile the public into another fear-fueled frenzy in order to justify the WHO’s takeover of public health globally, usher in those reviled health passports and everything else that goes along with The Great Reset. As noted by Hinchliffe in a 2020 Sociable article:41
“If you are World Economic Forum (WEF) Founder Klaus Schwab, you attempt to sell your vision of a global Utopia via a great reset of the world order in three simple steps:
1. Announce your intention to revamp every aspect of society with global governance, and keep repeating that message
2. When your message isn’t getting through, simulate fake pandemic scenarios that show why the world needs a great reset
3. If the fake pandemic scenarios aren’t persuasive enough, wait a couple months for a real global crisis to occur, and repeat step one ...
The so-called ‘great reset’ promises to build ‘a more secure, more equal, and more stable world’ if everyone on the planet agrees to ‘act jointly and swiftly to revamp all aspects of our societies and economies, from education to social contracts and working conditions.’
But it wouldn’t have been possible to contemplate materializing such an all-encompassing plan for a new world order without a global crisis, be it manufactured or of unfortunate happenstance, that shocked society to its core.”
COVID simply didn’t take the globalist cabal far enough. So, here comes global pandemic No. 2 — be it real or mostly fabricated — which will be rapidly followed by renewed calls for a New World Order and a Great Reset. Essentially, we can expect a repeat of the insanity we just lived through, which means we must also repeat our response, and reject the fearmongering and the global power grab.
In this interview, Dr. Nasha Winters, coauthor of “Mistletoe and the Emerging Future of Integrative Oncology,” reviews some of the benefits of this ancient herb in the modern world of oncology. Winters is herself a cancer survivor, so this topic is close to her heart.
“I'm coming on 30 years out of a death sentence, a terminal cancer diagnosis,” she says, “and still to this day get met with so much resistance to what I've learned for myself, and for thousands, if not tens of thousands, of other patients directly, as well as way more than that, indirectly, through the training of their physicians ...
My crazy controversy is that I focus more on the human organism and the health of that terrain versus the condition, the disease or the label that overlays that person.”
Mistletoe Has a 100-Year Oncological History
Mistletoe, a semi-parasitic plant that grows in the branches of trees all over the world, has been used as a herbal medicine for thousands of years for conditions such as epilepsy, spleen disorders, pain and rheumatic conditions.
Just over 100 years ago, in 1917, Rudolf Steiner, a philosopher with incredibly keen observation skills, noticed the mistletoe looks a lot like a tumor, and proposed it might have anticancer properties. Many vitalistic medical practices, such as Ayurveda, Chinese medicine, naturopathy and homeopathy, for example, use the doctrine of signatures, which is what Steiner was suggesting.
“For instance, you look at a walnut and it kind of looks like a brain and we think, I wonder if that's any good for the brain? And sure enough, we find some significance in how it impacts the brain. Or things like lungwort. When you look at it, it looks like a lung and we've learned that this herbal medicine is very helpful for lung conditions,” Winters says.
A Swiss doctor named Ita Wegman applied Steiner’s observation of mistletoe to see how it would impact a patient with cancer, and the plant has since enjoyed over 100 years of consistent application in oncology, both standalone and as adjuvant support.
“Interestingly enough ... Steiner understood that you needed to harvest different components of the plant — berries that bloom in the winter, which is very abnormal, and the leaves that grow in the summer ... and grow inward.
It has a very interesting behavior compared to other plants, and that was an observation of how cancer works as well. It goes against the rhythm. It grows out of sync with the organism. That is very much what he recognized.
And as such, he harvested the plant and aspects of the plant at different times, blended it, and then took a particular extract from it. He also noted that it needed to be injected, because you need to remember, 100 years ago we didn't know about lectins, we didn't know about viscotoxins, yet somehow, he understood that you needed to inject it to get the anticancer benefit.
You could take the full tincture. You could take it in other ways, and it has a lot of other medicinal impacts, but then it doesn't have the anticancer impacts, the reason being, we've learned — or at least we suspect, because we're still learning — is that those lectins and things get broken down in our GI tract and they don't get into the bloodstream; they don't access the immune system in the way they need to ...”
Mistletoe Can Be Used as an Adjunct for All Cancers
According to Winters, mistletoe is likely to be useful as an adjunct therapy for all cancers, and she, along with several other doctors, has been training physicians on how to use mistletoe for several years now.
“One of our physicians has been using mistletoe for 45 years in his practice, and what we've seen clinically, and what the research suggests, is that this therapy, it has always been about using it with others. It plays very well with others.
It was never really developed to be a standalone therapy, though believe me, we've seen impact with that as well. And it has virtually no contraindications with any of our standard of care therapies. So, we can literally inject this into a patient the morning before they go into a surgery, or they can start on this therapy the very day they're going to start a round of chemotherapy or radiation.
It bypasses first phase detox pathways of the liver, so it doesn't interact, intervene, speed up or slow down detox processes that could otherwise cause some adverse events, or change the desired effect of a certain medication, herbal intervention or dietary intervention.”
Mistletoe Is a Key Cancer Treatment Adjunct
In fact, mistletoe has been shown to enhance other interventions. Even the most toxic treatments seemingly work better and with fewer adverse effects when combined with mistletoe.
“This should be utilized, in my personal opinion, with every patient going through a standard of care approach to just enhance their experience with treatment,” she says.
“There are a lot of things that we kind of have to be careful with ... but mistletoe, in my experience, and that of my colleagues, is that this is probably the least harmful and least contraindicated substance and therapy I've ever had the privilege of working with. It’s pretty extraordinary and rare to find something that is this applicable to the masses ...
As I said, it has over 100 years of continuous use, and has over 250 very good randomized studies ... It just completed a Phase 1 clinical trial at John's Hopkins in the United States as an IV application for solid tumors, and is getting ready to be moved into a Phase 2 clinical trial.
It is the most studied integrative oncology therapy in the world, and it is utilized in upwards of 60% to 80% of all cancer patients in Europe. In parts of South and Central America, all over Southeast Asia and India, in different parts of Europe, this is just part of their medical system ... It's just in the United States where we have a little bit of resistance to embracing it into our conventional medical system ...
As a naturopathic physician who's been practicing integrative oncology for some time and who has teachers, mentors, colleagues from all over the world, some of the most powerful anticancer therapies I've seen that are beneficial even to the standard of care model of treatment — things like artesunate, curcumin, quercetin, green tea extract, all of those in intravenous forms — have been taken out of our ability to use here in the United States.
Do my colleagues still find workarounds to get access to these very important medicines? Absolutely they do, but they have to tread very carefully and very lightly. But again, you go north of the border or south of the border and you have no problem accessing these therapies. Or go to Europe — and this is what I've been doing for the last two years.
These treatments that we've had great success with have been plucked out of our ability to access easily, readily, legally, so we're now having to send our patients abroad for them to actually get good cancer care.
That's what's really devastating to me. So, another part of my purpose and mission is to build an in-house residential research institute and integrative cancer hospital right here on our soil so we don't lose access and patients don't lose access [to helpful remedies].”
Arizona Research Facility
Winters is currently building that research institute in Arizona, which will be funded entirely by private donations and research grants. Thousands of patients are anxiously waiting for the doors to open. When asked if she isn’t worried our pro-pharma agencies might shut them down, she replies:
“We will be doing all of our due diligence to let people know that these are not FDA approved therapies, that people are coming into a research environment. They're either paying cash or they're getting grants based on their financial ability to help them cover this care.
We're doing it in a pretty open-minded medical state; Arizona has one of the broadest scopes of practice in the country. And we're also very close to our southern border with Mexico, so that if we do come up against someone shutting down one of our therapies for a bit, we are able to take our patients across the border to a little sister clinic to keep the continuity of care.
We don't anticipate that happening because people are coming as a buyer beware. They're coming being well-informed about who we are and what we're about. And frankly, we get thousands of inquiries a month from all over the world looking for this approach. The patients will drive this home.
It’s a mighty David versus Goliath story, especially now, but I also think the time is now because we have these acts, like the Right to Try Act, and because we do have more and more patients facing this diagnosis with grim outcomes.
And, a study that came out in the last year that looked at 17 years’ worth of conventional cancer treatments found that, overall, of the 96 different drugs they looked at, the average survival rate was 2.4 months. That is the reality and this is what's driving the clinical oncologists from around the world to sign up and take my course ...
So, there is this massive kind of underground movement that's starting to sprout and come above ground. That's happening. And frankly, mistletoe is one of the vehicles for that to happen ... Instead of trying to fix the model, we're just creating a new one.”
Another potential “back door” is to convince insurance companies that this is in their best interest. Mistletoe is a natural remedy and therefore cannot be patented, so there’s no incentive for the drug companies to pursue it. But insurance companies may support its use once they realize how much money they can save on hospitalizations, drug coverage and everything else.
Mistletoe Modulates Immune Function
Your immune system and metabolic function are both integral parts of addressing cancer, and mistletoe works on both. It’s important to recognize, however, that it’s not a magic bullet. If you’re eating a standard American diet and are metabolically dysfunctional, mistletoe is not going to be as effective as for someone who is also eating a healthy whole food diet and supporting their health in other ways.
That said, mistletoe is an immunomodulator. Immune therapies are all the rage right now, with a majority of research dollars being funneled into them. Yet the effectiveness rate for these therapies is less than 20%. In other words, they’re hardly a cure.
“A lot of folks have heard of Jimmy Carter's melanoma story that had metastasized to his brain. He took this immune drug, Keytruda. That's a checkpoint inhibitor. The most common drugs you'll hear about are things like Opdivo, Keytruda, PD-1, PDL1 inhibitors, those are checkpoint inhibitors, or CTLA-4 inhibitors, also a type of checkpoint inhibitor.
These are drugs that kind of pull the breaks off your immune system to go hog wild in treating the cancer. Now that seems like a great idea — unless you have underlying metabolic dysfunction, right? Hello! And then, if you have an underlying autoimmune condition, you are also someone who's likely going to have a not so positive response to these medications.
What I love about mistletoe is it comes in and it modulates that teeter-totter. It doesn't take the breaks off and make it go hog wild, and it doesn't suppress. It’s ... kind of adaptogenic in some ways. So, it behaves a little bit like a smart drug, in that it can sort of match itself to the individual.
It is not a protocol, it's a patient-driven process in that we look at the person's gender, we look at the tumor type, the tumor stage, the general condition of the patient, and then we consider the most appropriate host tree. The most common are the pine, the fir, and the apple tree hosts. Mistletoe [from these trees] tends to have the highest lectin content that have the highest anti-cancer content.
Then we look at the dosing frequency, and if we're going to do it subcutaneous, intravenous, intratumoral, intraperitoneal, et cetera, depending on where you live in the world and how we're going to pair it with other therapies, if at all. So, it is based totally on the individual and the individual's response.
We want the patient to have a little local reaction if they're injecting it. We want it to get a little redness, irritation and itchiness and maybe tenderness. We want it to raise the body's temperature a little bit ... The point is, we want to create this cytokine release at a very low-grade level. Whereas when we bring on an immune drug like Keytruda, it creates a cytokine release at an explosive level that can sometimes be fatal for patients.”
Other Mechanisms of Action and Synergies
Similar to drugs, mistletoe also has a systemic effect. It doesn’t target a specific receptor site. Instead, it’s a systemic terrain-centric approach. In its mechanisms of action, it's engaging with B-cells, T-cells, natural killer (NK) cells.
It will basically calm those that are acting overzealous, to prevent an excessive immune reaction, and activate those that are dormant or underperforming. Mistletoe also reduces inflammation, lowering your levels of C-reactive protein, interleukin-6, homocysteine, liver enzymes and more.
It also lowers vascular endothelial growth factor (VEGF), which can be important for certain cancers, and it lowers blood sugar and insulin. Winters also suspects mistletoe may be upregulating both the endorphin and the endocannabinoid system, so you’re getting stress modulation as well.
“So, it’s hitting all of what we call ‘The Terrain 10,’ from my previous book, ‘The Metabolic Approach to Cancer.’ I find that mistletoe tends to hit every one of those ... including epigenetic expression ... clean up of DNA.
We use it for people who've gone through radiation. We'll use it as a DNA stabilizer. We'll use it if people have taken a course of Cipro [and other fluoroquinolones] to help clean up the metabolic mayhem, the DNA damage that they cause. We know that it has some impact on insulin and IGF-1.
In our book, we have hundreds of references to all of the different mechanisms of action. My colleague, Dr. Paul Faust, [has written] a beautiful chapter on its direct impact on the immune system and all the nuances of that.
That chapter alone will illuminate for so many people why this therapeutic support and this therapeutic intervention is so helpful for the cancer patient, for prevention of cancer, for cleanup after cancer treatment ...
And the synergy, when you pair mistletoe with hyperthermia, like so many of my colleagues in Europe have been doing for the past 50 years, talk about the biggest bang for your buck. We see some pretty extraordinary outcomes.
I've had patients go to Europe with Stage 4 [cancer], metastatic disease everywhere, getting IV mistletoe along with local, regional and whole body high-heat hyperthermia that have put their cancer into complete remission in many cases, but at the very least, turning it back into a manageable disease process, and even more interesting, increasing the responsivity to other therapies again.”
More Information
The good news is the number of doctors trained in this therapy is growing, and the treatment itself is only between $200 and $300 a month, so it’s highly affordable while also being highly effective. I think it would be beyond irrational not to integrate this into any cancer therapy you're considering.
Again, for cancer, oral supplementation is ineffective, as the lectins responsible for the anticancer effects are broken down in your GI tract and therefore can’t enter your bloodstream.
The Physicians' Association for Anthroposophic Medicine (PAAM) sponsors Winters’ mistletoe trainings. While most are held in person, there’s now also a course available online for licensed physicians. There are plans to take a group of physicians to Europe for immersive in-hospital training in the fall of 2023. Here’s a list of resources where you can find more information:
• Clinicians interested in training, visit the education section of PAAM’s website. The next annual training conference will be held in Loveland, Colorado, April 29 through May 6, 2023.
•Metabolic Terrain Institute of Health (MTIH) is the not-for-profit association cofounded by Winters that is building a research hospital in Arizona. MTIH also offers a master course for practitioners, and grants to help patients access these therapies. Certified practitioners can be found on terrain.network.
These practitioners include medical doctors and oncologists who have been taught Winters’ methodology of testing, assessing and treating cancer (which includes but is not limited to mistletoe therapy). MTIH certified practitioners are also listed on DrNasha.com.
•Mistletoe-therapy.org is a European website that offers helpful information for patients and scientific papers directed at clinicians.
• A load of resources are found on the book’s website: www.themistletoebook.com. Proceeds from this book go to fund clinical research and contribute to physician training.