Health, Fitness,Dite plan, health tips,athletic club,crunch fitness,fitness studio,lose weight,fitness world,mens health,aerobic,personal trainer,lifetime fitness,nutrition,workout,fitness first,weight loss,how to lose weight,exercise,24 hour fitness,
Labels
Technology
New Post
[recent][newsticker]
April 2022
Top Health News -- ScienceDaily
Aging
Alzheimer's
Articles
Articles : Asthma
Articles : CAFO
Articles : Children's Health
Articles : Cholesterol
Articles : Emotional Health
Articles : Fibromyalgia
Articles : GMO
Articles : Heart Health
Articles : Hormones
Articles : Internal Videos
Articles : Interviews
Articles : Men's Health
Articles : Politics
Articles : Thyroid Disease
Articles : Vaccines
Autism
best natural health source
Children's Health
Detoxification
Diabetes
Diet | body+soul
Diet and Weight Loss News -- ScienceDaily
Digestive Diseases
Dite
Dite & weight loss
Drug Industry
Drugs
EFT
EMF
Emotional Health
Finances
fitness
Fitness | body+soul
Fitness/Exercise
Fluoride
Food
Fructose/Sugar
Gardening
Harvard Health Blog
Health
Health | body+soul
Health and Wellness
health news
health tips
Heart Health
information
Joint Support
Juicing
Men's Health
news
Nutrition
Nutrition | body+soul
Pollution
Raw Milk
Soy
Supplements
Swine Flu
Technology
Thyroid Disease
Top Health
Top Health News -- ScienceDaily
Under Armour
Vaccines
Weight Management
women's health
Women's Health News -- ScienceDaily
work place health
Workplace Health News -- ScienceDaily
A new mutation behind synucleinopathies
Scientists have carried out an extensive study of a newly discovered mutation that can uncover new insights into the molecular basis of pathology formation in a family of disorders that includes Lewy body dementia and Parkinson's disease.
from Top Health News -- ScienceDaily https://ift.tt/qD1kryF
from Top Health News -- ScienceDaily https://ift.tt/qD1kryF
High-frequency spinal cord stimulation shows improved longer lasting pain relief
Researchers at UC San Diego School of Medicine report that high-frequency spinal cord stimulation proved more effective at improving perceived pain reduction than low-frequency SCS in patients studied, and that there was some variation in PPR between male and female patients.
from Top Health News -- ScienceDaily https://ift.tt/JAYbT34
from Top Health News -- ScienceDaily https://ift.tt/JAYbT34
Unlocked enzyme structure shows how strigolactone hormone controls plant growth
As sessile organisms, plants have to continually adapt their growth and architecture to the ever-changing environment. To do so, plants have evolved distinct molecular mechanisms to sense and respond to the environment and integrate the signals from outside with endogenous developmental programs. New research unravels the underlying mechanism of protein targeting and destruction in a specific plant hormone signaling pathway.
from Top Health News -- ScienceDaily https://ift.tt/H6OJpnP
from Top Health News -- ScienceDaily https://ift.tt/H6OJpnP
Gut microbiome may alter response to cancer therapy
A new study captures the current understanding of the connection between the gut microbiome and therapeutic response to immunotherapy, chemotherapy, cancer surgery and more, pointing to ways that the microbiome could be targeted to improve treatment.
from Top Health News -- ScienceDaily https://ift.tt/YHE4zTj
from Top Health News -- ScienceDaily https://ift.tt/YHE4zTj
All cells are important: A roadmap to characterize lymphoma stroma
Researchers identify gene expression signatures in different types of lymph nodes cells that play an active role in the development of lymphomas.
from Top Health News -- ScienceDaily https://ift.tt/eGN7nEY
from Top Health News -- ScienceDaily https://ift.tt/eGN7nEY
Scientists illuminate mechanism of common drug target
Using advanced imaging methods, researchers have gained insight into how a common target of drugs sends cellular signals, a finding that may lead to better and more precise therapeutics.
from Top Health News -- ScienceDaily https://ift.tt/7OiGsyp
from Top Health News -- ScienceDaily https://ift.tt/7OiGsyp
Study tracks COVID-19 infection dynamics in adults
Scientists tracked the rise and fall of SARS-CoV-2 in the saliva and nasal cavities of people newly infected with the virus. The study was the first to follow acute COVID-19 infections over time through repeated sampling and to compare results from different testing methodologies.
from Top Health News -- ScienceDaily https://ift.tt/0Jp46UH
from Top Health News -- ScienceDaily https://ift.tt/0Jp46UH
CAR T drives acute myeloid leukemia into submission in pre-clinical studies
Investigators have devised a novel method for improving CAR T therapy through a drug combination and cellular engineering that improves the strength and durability of the tumor-killing effect of a CAR T directed against acute myeloid leukemia.
from Top Health News -- ScienceDaily https://ift.tt/DJoHS7Y
from Top Health News -- ScienceDaily https://ift.tt/DJoHS7Y
CAR-T therapy effective in Black and Hispanic patients
CAR-T therapy, a form of immunotherapy that revs up T-cells to recognize and destroy cancer cells, has revolutionized the treatment of blood cancers, including certain leukemias, lymphomas, and most recently, multiple myeloma. However, Black and Hispanic people were largely absent from the major clinical trials that led to the U.S. Food and Drug Administration approval of CAR-T cell therapies.
from Top Health News -- ScienceDaily https://ift.tt/v4eUR3E
from Top Health News -- ScienceDaily https://ift.tt/v4eUR3E
Selection bias may lead to underestimation of risk of CTE in former football players
Researchers have been studying chronic traumatic encephalopathy (CTE) and while much has been learned, diagnosing the disease still needs to be done post-mortem on autopsied brains donated to a brain bank. One criticism of the research is that brain bank study results have a selection bias because they are based on a subset of players most affected by CTE, and therefore not representative of the population of football players. Now a novel study by researchers from BUSM and Boston University School of Public Health (BUSPH) provides further evidence suggesting a dose-response relationship between football and CTE even after adjusting for selection bias.
from Top Health News -- ScienceDaily https://ift.tt/az0qUZO
from Top Health News -- ScienceDaily https://ift.tt/az0qUZO
Aspirin does not cut risk in non-obstructive coronary artery disease, study finds
Aspirin therapy, as opposed to statin use, for non-obstructive coronary artery disease does not reduce major cardiovascular events, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/ynGWqd1
from Top Health News -- ScienceDaily https://ift.tt/ynGWqd1
From blurry to bright: AI tech helps researchers peer into the brains of mice
Biomedical engineers have developed an artificial intelligence (AI) training strategy to capture images of mouse brain cells in action. The researchers say the AI system, in concert with specialized ultra-small microscopes, make it possible to find precisely where and when cells are activated during movement, learning and memory.
from Top Health News -- ScienceDaily https://ift.tt/CGquAiO
from Top Health News -- ScienceDaily https://ift.tt/CGquAiO
New study identifies genetic changes in patients who progress to esophageal cancer
A scientific team who studies a precancerous condition of the esophagus (called Barrett's esophagus or BE) are working to answer how to see genetic changes in cells before they turn cancerous. The team revealed that DNA changes in BE cells that presage esophageal cancer can be spotted years before cancer develops.
from Top Health News -- ScienceDaily https://ift.tt/iZfltMD
from Top Health News -- ScienceDaily https://ift.tt/iZfltMD
Genetic diversity of C. difficile, a particularly problematic pathogen
Researchers have used a systems biology approach to parse the genetic diversity of Clostridioides difficile, a particularly problematic pathogen, particularly in health care settings.
from Top Health News -- ScienceDaily https://ift.tt/vwUdtVm
from Top Health News -- ScienceDaily https://ift.tt/vwUdtVm
A new polymer system to revolutionize the delivery of therapeutics
Researchers recently announced that they have engineered a new class of material, called a 'polyzwitterionic complex,' or 'pZC,' which is able to both withstand the harsh acidic conditions of the stomach and then dissolve predictably in the comparatively gentle environment of the small intestine. This property means that pZCs could help revolutionize the delivery of medicines of all sorts, from familiar oral antibiotics to new classes of delicate protein therapeutics.
from Top Health News -- ScienceDaily https://ift.tt/v7NpSHm
from Top Health News -- ScienceDaily https://ift.tt/v7NpSHm
Scientists implicate non-cardiac genes in congenital heart disease
Researchers show that three transcription factors -- GATA4, NKX2-5 and TBX5 -- interact with CHD4 inside the embryonic heart, recruit it for action, and uses CHD4 to play their roles in heart health and disease.
from Top Health News -- ScienceDaily https://ift.tt/W70oRSz
from Top Health News -- ScienceDaily https://ift.tt/W70oRSz
A refined microbiome 'fingerprint' method tracks sub-strain variants of a single gut microbe strain
A previously developed a microbiome 'fingerprint' method that identifies single strains of particular gut bacteria through analysis of metagenomics data from fecal samples, has been refined to include looking for single-nucleotide variants in the KEGG metabolic pathways of a particular strain. This magnified analysis shows a short-term difference in sub-strain dynamics of two Bacteroides species between healthy individuals and hospitalized COVID-19 patients.
from Top Health News -- ScienceDaily https://ift.tt/v1eQzEI
from Top Health News -- ScienceDaily https://ift.tt/v1eQzEI
Japanese population projected to live longer without dementia
A new microsimulation projects that over the next 20 years, Japanese people will live longer without dementia, but older women with a less than high school education will benefit less than men.
from Top Health News -- ScienceDaily https://ift.tt/4BumYsT
from Top Health News -- ScienceDaily https://ift.tt/4BumYsT
Neuronal plasticity in chronic pain-induced anxiety revealed
Researchers have shown how chronic pain leads to maladaptive anxiety in mice, with implications for treatment of chronic pain-related psychiatric disorders in humans.
from Top Health News -- ScienceDaily https://ift.tt/efaISsv
from Top Health News -- ScienceDaily https://ift.tt/efaISsv
Better assess the needs of people with multiple disabilities
How do we assess the needs of people with severe multiple disabilities? Unable to communicate verbally and physically, this population has nearly no possibility of expressing itself. Thanks to eye-tracking technology, a team has succeeded in identifying and evaluating certain perceptive and social-emotional abilities in nine children and adolescents with multiple disabilities, opening the way to personalized care.
from Top Health News -- ScienceDaily https://ift.tt/gcZknyV
from Top Health News -- ScienceDaily https://ift.tt/gcZknyV
Scientists identify chemical markers that may unlock future therapeutic uses of mRNA
Researchers set out to find new ways to artificially induce mRNA to respond in ways that could eventually lead to therapeutic outcomes, expanding on the success of the mRNA-based COVID-19 vaccines and opening up new possibilities across a host of possible genetic therapies.
from Top Health News -- ScienceDaily https://ift.tt/4OsrGKl
from Top Health News -- ScienceDaily https://ift.tt/4OsrGKl
Learning chemical networks give life a chiral twist
A study shows that the preference of biological molecules for left or right-handedness -- a hallmark of living matter -- could emerge spontaneously as prebiotic chemical networks adapt to optimize energy harvesting. The proposed mechanism of symmetry breaking is general and can apply to other transitions in living matter that lead to increased complexity.
from Top Health News -- ScienceDaily https://ift.tt/Bzvbtx0
from Top Health News -- ScienceDaily https://ift.tt/Bzvbtx0
Study suggests early self-awareness of autism leads to better quality of life
People who learn they are autistic when they are younger may have a heightened quality of life and sense of well-being in adulthood, according to a new study.
from Top Health News -- ScienceDaily https://ift.tt/1UzOe4I
from Top Health News -- ScienceDaily https://ift.tt/1UzOe4I
Micronutrients (vitamins + minerals) show benefit for children with ADHD and emotional dysregulation
A study reports that children with ADHD and emotional dysregulation randomized to take a micronutrient formula were three times more likely to show symptomatic improvement on blinded clinician ratings, compared to those in the placebo group (54% versus 18%). The micronutrient formula, consisting of all known vitamins and essential minerals, was administered for eight weeks.
from Top Health News -- ScienceDaily https://ift.tt/5ey1YJm
from Top Health News -- ScienceDaily https://ift.tt/5ey1YJm
A new treatment reduces inflammation in multiple sclerosis mice models
Researchers managed to reduce chronic inflammation associated with multiple sclerosis in mice thanks to the administration of a type of lipid that mediates inflammation.
from Top Health News -- ScienceDaily https://ift.tt/r7AKIUX
from Top Health News -- ScienceDaily https://ift.tt/r7AKIUX
Boys are more demanding than girls before they are born, according to scientists
Finding out the sex of a baby during pregnancy could lead to better life chances, a new study has discovered. Male baby pregnancies are more likely to result in complications, possibly because they grow faster in the womb and require more nutrients and oxygen than supplied by the mother through the placenta -- the temporary organ that attaches to the wall of the uterus during pregnancy to help the fetus grow and develop.
from Top Health News -- ScienceDaily https://ift.tt/vo5wy2d
from Top Health News -- ScienceDaily https://ift.tt/vo5wy2d
Offspring weakens when parents are given antibiotics
New study shows the immune system of zebrafish weakens if one parent has been exposed to antibiotics. Antibiotics can have unwanted effects for several generations, researchers discover.
from Top Health News -- ScienceDaily https://ift.tt/R5AaI12
from Top Health News -- ScienceDaily https://ift.tt/R5AaI12
Firearms kill more children than car crashes, new report finds
In an analysis of the most recent data available through the CDC, clinical researchers revealed that firearm injuries are now the leading cause of death among children up to age 19, and the racial gap between black and white youth is widening. The article calls for health care workers to recognize this as an epidemiological and public health challenge and to help find solutions.
from Top Health News -- ScienceDaily https://ift.tt/dA1SJox
from Top Health News -- ScienceDaily https://ift.tt/dA1SJox
Scientists discover mechanism behind chemically induced suppression of fearful memories
Fearful events negatively impact the brain. For instance, war veterans often go through post-traumatic stress disorder months after the cessation of the triggering event. Now, the precise mechanism of suppression of such fearful memories has been uncovered. Using a mouse model, the researchers identified the associated biochemical pathways, thus paving the way for the development and clinical evaluation of therapeutic compounds such as KNT-127.
from Top Health News -- ScienceDaily https://ift.tt/sfHNeTr
from Top Health News -- ScienceDaily https://ift.tt/sfHNeTr
Omega-3 and Vitamin D May Reduce Heart Failure Complications
Data from a study1 published in April 2022 in JACC: Heart Failure reveals that people with Type 2 diabetes who used omega-3 supplements had a lower incidence of hospitalization with heart failure. Heart failure is a form of heart disease in which the heart experiences ventricular dysfunction.
The heart is separated into four chambers. The bottom two chambers called the ventricles, pump blood to the lungs or the body.2 When there is left ventricular failure, a person experiences fatigue and shortness of breath. With right ventricular failure a person may experience abdominal and peripheral fluid buildup.
Heart failure can affect one or both sides of the heart. Experts believe there are more than 15 million new diagnoses of heart failure globally each year.3 In the U.S., more than 600,000 new cases are diagnosed each year. Additionally, it's estimated that 10 times that number of Americans currently have heart failure.
Despite advances in drug therapy, the prognosis continues to remain poor. Individuals with severe heart failure have a mortality rate of up to 60% over one year and up to 30% mortality rate in mild to moderate failure.4 Heart failure develops as the ventricles become inefficient. This can happen from a variety of different factors that place excessive demand on the heart.
One factor that can lead to heart failure is long-term, uncontrolled high blood pressure or hormonal disorders such as hyperthyroidism. But, the primary cause of heart failure is coronary artery disease, which reduces the delivery of oxygen and nutrients to the heart muscle. Over time, this leads to impaired function.
There's also a relationship between chronic high blood pressure and coronary artery disease,5 which means that high blood pressure may have an effect on the development of heart failure through at least two pathways. The primary focus of the featured study was to evaluate whether an omega-3 supplement could reduce the risk of hospitalization for heart failure in participants with or without Type 2 diabetes.
Omega-3 Supplements Lower Risk of Heart Failure Admission
The data were gathered from the vitamin D and omega-3 trial (VITAL)6 that started in 2010. VITAL, the parent trial for this study, engaged 25,871 men and women to evaluate their dietary supplementation of vitamin D3 or omega-3 fatty acids and the impact it had on developing heart disease, stroke or cancer in people who did not have a history of these health conditions.
Participants took the supplements for a five-year intervention phase and researchers have continued with ongoing follow-up. The ancillary study began in 2014, in which the researchers assessed the role that race and Type 2 diabetes had on supplementation with omega-3 fatty acids.
There were four arms to the study.7 The first group received 2,000 international units (IU) per day of vitamin D3 and 1 gram per day of fish oil. The researchers compared results against three other groups who received either two placebos, or a placebo for vitamin D or fish oil. The primary outcome measure was new heart failure with hospitalization and the secondary outcome measure was recurrent hospitalization.
When the researchers evaluated the results8 they found that omega-3 supplements could reduce hospitalization rate for the first heart failure by 0.69 in participants who had Type 2 diabetes when compared to taking a placebo. They also found that omega-3 effectively reduced recurrent hospitalization in black participants. The results did not show a benefit for individuals who did not have Type 2 diabetes.
However, the researchers did not measure the omega-3 index for these individuals, thus it is difficult to determine if omega-3 levels were low in those who experienced the greatest benefit. There is evidence to suggest from past studies that individuals with Type 2 diabetes have significantly lower omega-3 indices than those who do not have Type 2 diabetes,9 suggesting increasing dietary intake may help prevent the condition.
Data10 also suggests that omega-3 supplementation may help lower inflammatory levels in people with diabetes, which also contributes to better heart health.11
Vitamin D Significant Factor in Heart Failure Outcomes
One arm of the study included participants who took only vitamin D and a placebo to replace omega-3 fatty acids. In this cohort, the researchers did not find that only vitamin D could help reduce hospitalization rates in people with heart failure. However, there is evidence from multiple past studies that vitamin D has a significant effect on protecting heart health.
Data from one study showed an anti-inflammatory effect from vitamin D in patients with congestive heart failure (CHF) suggesting it may serve as “a new anti-inflammatory agent for the future treatment of the disease. Our data provide evidence for the involvement of an impaired vitamin D–parathyroid hormone axis in the progression of CHF.”12
Evidence also suggests that vitamin D has an impact on mineral metabolism and myocardial dysfunction in patients with CHF. Researchers wrote in the American Journal of Cardiology that deficiency may be “a contributing factor in the pathogenesis of CHF.”13
Epidemiological studies have also provided strong support that vitamin D has cardioprotective effects14 and data also show that most patients with CHF have insufficient vitamin D levels, lower than 20 ng/mL.15 Researchers hypothesize that this may be related to the sedentary lifestyle of people with CHF and that insufficient levels contribute to the etiology of the disease.
More data indicated that low concentrations of vitamin D3 contribute to a poor prognosis in patients with heart failure, which may be related to inflammation.16 Furthermore, deficiency is highly prevalent, including in patients with heart failure and is “a significant predictor of reduced survival.”17
Researchers found that supplementing with vitamin D was independently associated with a reduction in mortality and that lower vitamin D levels were associated with high body mass index, diabetes, decreased calcium and hemoglobin levels and female gender.18
Sulfur and Magnesium: Two Crucial Nutrients for Heart Health
Sulfur has been a “forgotten” nutrient and you don't hear it mentioned very often. Yet it's very important for optimal body function and health. You get most of your sulfur from certain proteins in your diet, specifically, those that contain the amino acids methionine, cysteine, cystine, homocysteine, homocystine and taurine.19 Of these, the two most important are methionine and cysteine.
Neither of these is stored in the body, although glutathione is a key storage form of sulfur.20 Glutathione keeps many other antioxidants performing at peak levels and cysteine availability is thought to be a rate-limiting factor for glutathione synthesis.21 According to Stephanie Seneff, Ph.D., who has written several papers on sulfur,22,23,24 deficiency appears to play a role in a wide range of health problems and diseases, including heart disease.
In 2011, during an interview with Seneff,25 we discussed the influence that sulfur has on health and disease. She talked about the crucial connections between sulfur, cholesterol and vitamin D, suggesting that sensible sun exposure plays an important role in heart and cardiovascular health as it regulates not only vitamin D3 but also cholesterol sulfate in circulation.
Magnesium also plays a crucial role in high blood pressure and cardiovascular disease. Because serum magnesium is not a reflection of the total amount your body has available, experts believe that most cases of deficiency go undiagnosed.26 Additionally, because of a decrease of magnesium in the soil, medications and the number of processed foods eaten by the majority of people, many are at risk for deficiency.
Low levels of magnesium have been associated with Type 2 diabetes, high blood pressure, atherosclerotic vascular disease and sudden cardiac death.27 Some estimates are that nearly half the U.S. population eats less than the required amount of magnesium-rich food and that the prevalence and incidence of Type 2 diabetes rose while consumption of magnesium declined.
Magnesium is a natural calcium channel blocker that also increases nitric oxide production to relax the arteries and improve endothelial dysfunction.28 These functions reduce the risk of high blood pressure.29
Researchers have been studying the effect of magnesium on blood pressure for many years, but not always with the same results. One literature review of 44 human trials proposes that the dissimilar results are a function of study designs that are not uniformly matched between studies.30 When a uniform subset of the 44 studies was combined, the scientists found a strong effect of magnesium against high blood pressure.
Low Sodium Diet Increases Risk of Heart Failure
In this video, James DiNicolantonio, Pharm.D, discusses the parallel between the rise of high blood pressure, diabetes and obesity with the reduction in salt consumption that began in the early 1900s. He goes on to explain that one of the body's ways of retaining salt is to increase insulin. With a low salt intake, your body becomes insulin resistant, which helps explain the rise in triglyceride levels in people who eat a low salt diet.
Guy Johnson, Ph.D., principal at Johnson Nutrition Solutions LLC, filed a petition with the FDA to request a qualified health claim for conventional foods and dietary supplements that contain 20% of the daily value of magnesium.31 He proposed, based on hundreds of studies and papers,32 that magnesium could reduce the risk of high blood pressure.
Six years later, in January 2022,33 the FDA responded with a 42-page letter,34 in which they concluded there wasn't enough evidence35 after reviewing just 38 intervention studies. After documenting their reasons for discounting the results, the letter identified a secondary factor that must be met for the qualified health claim to be used — the conventional foods must also meet the “low sodium” criteria, writing:36
“Sodium attracts water, and a high-sodium diet draws water into the bloodstream, which can increase the volume of blood and subsequently your blood pressure. High blood pressure or hypertension is a condition that makes the heart work too hard, and the high force of the blood flow can harm arteries and organs (such as the heart, kidneys, brain, and eyes).”
However, this is a rather simplistic view of how the body works. Sodium balance is impacted by several nutrients and kidney health. Your body uses magnesium, calcium37 and potassium38 to balance sodium, which in turn affects other aspects of your health, such as bone destiny, blood pressure, and heart and kidney health. When one level changes, it affects the others.
Sodium restriction has been a cornerstone of heart failure management. To move the focus to the other more damaging white crystal — sugar39 — one paper40 from Rush University Medical Center found salt restriction was associated with an increased risk of heart failure and death.
A second study41 demonstrated the risk of cardiovascular events decreased as the potassium level increased. There have been hundreds of studies across nearly every bodily system that shows maintaining overall health is not a singular function but, rather, a complex interaction between nutrients, enzymes and bodily systems.
Sleep Is Another Factor That May Raise Risk of Heart Disease
Your heart health depends on multiple factors, including how many hours of sleep you get each night. Researchers with the National Center for Cardiovascular Research42,43 in Madrid, Spain found people who slept less than six hours each night were 27% more likely to have subclinical atherosclerosis than those who slept for seven or eight hours each night.
Subclinical atherosclerosis can trigger congestive heart failure as it increases the exercise load on the heart muscle. People who have fragmented sleep, which means they wake up often or have trouble falling asleep, also had a 34% increased risk of subclinical atherosclerosis compared to longer sleepers.44 In the study, the researchers found there was a sweet spot since sleeping either too little or too much increased risk.
Women who slept for more than eight hours a night doubled the risk of subclinical atherosclerosis compared to those who slept seven or eight hours each night. The participants who were an average age of 46 years had a 5.9% risk of having a heart attack or stroke in the next 10 years or 17.7% in the next 30 years.45 Yet, when the women slept for less than six hours a night, that risk increased to 6.9% for 10 years and 20.9% for 30 years.
“[T]his study emphasizes we have to include sleep as one of the weapons we use to fight heart disease — a factor we are compromising every day,” senior study author José M. Ordovás, Ph.D., said.46 What’s more, he added, “This is the first study to show that objectively measured sleep is independently associated with atherosclerosis throughout the body, not just in the heart.”
The link between sleep and heart health is not new, and it could be that even seven hours is just barely enough. People who sleep less than seven hours a night have an increased risk of heart disease,47 and this is true regardless of other factors that influence heart health, like age, weight, smoking and exercise habits.
People who struggle with sleep apnea, which causes frequent nighttime awakenings, often have heart trouble as well. Women with sleep apnea tend to have higher levels of the protein troponin T, which is a marker for heart damage and are more likely to have an enlarged heart,48 which is a risk factor for heart failure. Too little sleep may also increase the inflammation in your body.
"Sleep-deprived people have higher blood levels of stress hormones and substances that indicate inflammation, a key player in cardiovascular disease. Even a single night of insufficient sleep can perturb your system,” according to Dr. Susan Redline, of the Division of Sleep Medicine at Harvard Medical School.49
Lack of sleep also increases your risk of several health problems that take a toll on heart health, including high blood pressure, Type 2 diabetes and obesity, which are all risk factors for heart failure.
from Articles https://ift.tt/rf56jB8
via IFTTT
Another Layer of Corruption in the Opioid Scandal Revealed
In 2021, McKinsey & Company, one of the largest consultants to corporations and governments worldwide, settled a lawsuit brought by 47 state attorneys general over its role in the U.S. opioid crisis. The firm agreed to pay $573 million in fines1 for driving up sales of Purdue Pharma’s OxyContin painkiller, even as Americans were dying in droves.
Between 1999 and 2019, nearly 500,000 Americans died from overdoses involving opioid drugs,2 and false advertising and bribery were at the heart of this tragedy. As reported by The New York Times:3
“McKinsey’s extensive work with Purdue included advising it to focus on selling lucrative high-dose pills, the records show, even after the drugmaker pleaded guilty in 2007 to federal criminal charges that it had misled doctors and regulators about OxyContin’s risks. The firm also told Purdue that it could ‘band together’ with other opioid makers to head off ‘strict treatment’ by the Food and Drug Administration.”
Worse Than We Thought
We now find out that the situation is even more corrupt than we previously thought. A U.S. House investigation4,5,6 into McKinsey, based on materials obtained through the discovery process of this and other lawsuits, has revealed McKinsey was advising the FDA on the safety of opioids, while at the same time advising Purdue how to maximize sales.
In one instance, McKinsey wrote “scripts” for Purdue to use in its meeting with the FDA to discuss the safety of OxyContin in pediatric populations. In another, Jeff Smith, a senior McKinsey consultant, worked on a risk evaluation and mitigation strategy (REMS) for OxyContin while simultaneously advising the FDA about the drug’s safety.7
As noted by investigative journalist Paul Thacker,8 “Just think about that for a moment — for years McKinsey played both cop and robber.” As reported by The New York Times, April 13, 2022:9
“Since 2010, at least 22 McKinsey consultants have worked for both Purdue and the FDA, some at the same time, according to the committee’s 53-page report ...
The firm provided no evidence to the committee that it had disclosed the potential conflicts of interest as required under federal contracting rules — an ‘apparent violation,’ the report said.
McKinsey also allowed employees advising Purdue to help shape materials that were intended for government officials and agencies, including a memo in 2018 prepared for Alex M. Azar II, then the incoming secretary of health and human Services under President Donald J. Trump.
References to the severity of the opioid crisis in a draft version of the memo, the documents show, were cut before it was sent to Mr. Azar.
‘Today’s report shows that at the same time the FDA. was relying on McKinsey’s advice to ensure drug safety and protect American lives, the firm was also being paid by the very companies fueling the deadly opioid epidemic to help them avoid tougher regulation of these dangerous drugs,’ Representative Carolyn Maloney, the New York Democrat who chairs the committee, said in a statement ...
A bipartisan group of lawmakers last month introduced legislation10 aimed at preventing conflicts of interest in federal contracting, citing McKinsey’s experience with Purdue and the FDA.”
The FDA, in response, has stated that it “relies on its contractors to assess and report potential conflicts of interest,” The New York Times reports.11 In other words, it’s just pointing fingers and refusing to take responsibility for working with advisers that clearly could, and should, be suspected of having ulterior motives, based on their client base.
Isn’t it obvious that McKinsey, working to improve sales for its opioid-making clients, might give the FDA biased advise on behalf of those clients? Remarkably, in October 2021, the FDA wrote12 to senators claiming they had no idea McKinsey was even working for Purdue, and didn’t find out about it until media reported it in early 2021.
It seems beyond irrationally foolish that the press could find out about it, but not the FDA — somewhat like the head of the CDC, Dr. Rochelle Walensky, going on CNN and quoting Pfizer press releases as factual data.
McKinsey Advised FDA on Opioid Safety
The FDA hired McKinsey as an adviser in 2011. The company worked with the FDA office overseeing drug companies plans to monitor safety of risky products such as opioids, and internal documents show that, on multiple occasions, McKinsey promoted its FDA connections when pitching services to its pharmaceutical clients.13
For example, in a 2009 sales pitch, McKinsey wrote that it provided direct support to regulators, “and as such have developed insights into the perspectives of the regulators themselves.”14
In a 2014 email to Purdue’s chief executive, McKinsey consultant Rob Rosiello wrote, “We serve the broadest range of stakeholders that matter for Purdue. One client we can disclose is the FDA, who we have supported for over five years.”15
Evidence also suggests McKinsey took “steps to limit material that could be subpoenaed” once Purdue was sued, The New York Times reports.16 In one instance, printed hardcopies of slide decks were sent to Purdue instead of being emailed because they knew Purdue staff would be deposed and didn’t want their email correspondence to “get sucked into it.”
Did McKinsey Influence FDA Commissioner?
The Interim Majority Staff report17 by the Committee on Oversight and Reform, titled “The Firm and the FDA: McKinsey & Company’s Conflicts of Interest at the Heart of the Opioid Epidemic,” published April 13, 2022, also includes emails in which McKinsey employees claim to have influenced an opioid safety speech by then-FDA commissioner Dr. Scott Gottlieb.
Gottlieb denies the accusation, but the fact that McKinsey was working so intimately with the FDA means they certainly would have been capable of such influence. Gottlieb also has financial ties to the opioid industry, having received $45,000 in speaker’s fees from companies that manufacture and distribute opioids.18
In 2012, Gottlieb also wrote a Wall Street Journal essay, attacking the Drug Enforcement Administration (DEA) for pursuing the criminal activity of opioid distributors, saying it would burden patients, “including those with legitimate prescriptions who may be profiled at the pharmacy counter and turned away.”19
Intent to Harm
What we have here is a picture of gross conflicts of interest with an apparent intent to harm. Purdue Pharma was as crooked as they come, conducting sham studies and bribing doctors to prescribe its highly addictive opioid, while its consultant, McKinsey advised the FDA on the drug’s safety.
At the same time, Purdue also worked with the Publicis Groupe — the largest PR company in the world as of November 202120 — which funded the startup of NewsGuard, a “fact checking” group that rates websites on criteria of “credibility” and “transparency.” In April 2021, Publicis partnered with NewsGuard specifically “to fight the ‘infodemic’ of misinformation about COVID-19 and its vaccines.”21
NewsGuard’s health-related service, HealthGuard,22 is also partnered with the Center for Countering Digital Hate (CCDH) — a progressive U.K.-based cancel-culture leader23 with extensive ties to government and global think tanks that has labeled people questioning the COVID-19 vaccine as “threats to national security.”
At the beginning of May 2021, the Massachusetts attorney general filed a lawsuit24,25 against Publicis Health, accusing the Publicis subsidiary of helping Purdue create the deceptive marketing materials used to mislead doctors into prescribing OxyContin.26,27,28,29
Like Purdue, Publicis also cashed in on the opioid addiction it helped create by pitching its services to organizations working to end addiction. As reported by Forbes,30 the agency “won the account to work on drugfree.org after touting how it’s been ‘immersed in the evolving national opioid medication dialogue going on between pharma companies, the government and FDA, and the public via inside access as a trusted and informed consulting partner.’”
So, to summarize, Purdue knew the dangers of its drug, covered them up, hired FDA insiders to advise its sales strategy and influence the FDA, and is connected with a PR company that had the ability to suppress and censor negative news to manage its marketing. It’s hard to describe this scheme as anything but intentional mass murder.
The Spin Doctors
The reality may even be worse, and much larger, than that, seeing how Publicis is also a partner of the World Economic Forum (WEF),31 which is leading the call for a “reset” of the global economy and a complete overhaul of our way of life.32
As detailed in the featured video, Publicis’ fingerprints can be found throughout the net of censorship and misdirection that is now being cast across the digital landscape. As the No. 1 PR company in the world, Publicis has just the right credentials and influence to pull off a deception of this size.
It’s part of an enormous network that includes international drug companies, fact checkers and credibility raters, Google, Microsoft, public libraries, schools, the banking industry, the U.S. State Department and Department of Defense, the World Health Organization and Disney, just to name a few. As noted by investigative reporter David Marks in “How PR Giant Publicis Promotes Greed, Deception on Behalf of World’s Most Powerful”:33
“The essential skill of these expert spin doctors is their ability to fabricate a favorable interpretation of damaging information or activity or diminish the impact of the truth.
Through tried and true psychological ploys, repetition of false information or casting doubt on factual realities, ad agencies and PR firms target those who need to be influenced on behalf of their clients ...
An examination of one of the largest entities neck-deep in managing these mass psychological operations reveals the depth of the dysfunction afflicting the planet. The vast activities of the Publicis Groupe demonstrate how the tentacles of greed, profit and privilege connect the catastrophic agendas of the most powerful enterprises on Earth ...
Using sophisticated social psychology and incorporating the cutting edge of artificial intelligence, Publicis PR experts are masters of damage control, the manipulation of words and people, and of selling the unsellable. Publicis is organizing influential activities worldwide, overtly revealing its mission and priorities.
... [Its] website reveals who actually benefits from the company's services: ‘The entire Publicis Groupe transformation was designed to put clients at the center of all we do. Their needs and objectives drive the solutions we provide in order to help them win and grow’ ...
In considering the range of activities Publicis engages in, the dots are so close there is no need to connect them. The PR giant's methodology is transparent.
Whether promoting opioids or pushing vaccines, rebranding status quo profiteering as a Great Reset, supporting cigarette sales, disguising the true nature of the fossil fuel industry, increasing soft drink consumption or covering for assassinations — Publicis has all the skills and facilities to create whatever fabrications are needed to sell products and influence how their wealthy collaborators are viewed.
The Publicis Groupe and its allies are at the hub of a worldwide insidious, destructive disinformation campaign, relying on the duplicitous ways of advertising and public relations in the loyal service of clients.”
A Plan to Drug the Useless Eaters?
As a WEF partner and global PR machine for some of the most powerful industries on the planet, it seems reasonable to assume Publicis is helping to coordinate the WEF’s Great Reset agenda. Sadly, that includes not only the management and control of the peoples of the earth, but also the elimination of “undesirables.”
In a 2015 interview (video above), Yuval Noah Harari, a history professor and adviser to WEF founder Klaus Schwab, discussed what Schwab refers to as The Fourth Industrial Revolution (i.e., transhumanism), noting that we’re now learning to “produce bodies and minds” (meaning augmented bodies, and cloud and artificial intelligence-connected minds) and that one of the greatest challenges we face will be what to do with all the people that have become obsolete in the process.
How will unaugmented people find meaning in life when they’re basically “useless, meaningless”? How will they spend their time when there’s no work, no opportunity to move up in some kind of profession? His guess is that the answer will be “a combination of drugs and computer games.”
This raises a disturbing question. Was the opioid crisis the result of an intentional plan — a conspiracy in the literal sense of the word — to hook the masses on an addictive drug? This is purely speculative, of course, but it surely fits in with The Great Reset agenda as a whole.
If people are addicted, the drug and medical industries make money (and they’re without doubt part of The Great Reset network), and if people die, well, that’s in accordance with The Great Reset plan too, as they insist there are too many “useless eaters” on the planet, and they either must be managed or eliminated.
Publicis Is Part of the Global Monopoly
In closing, it’s worth noting that Publicis is partially owned by the Vanguard Group,34 one of the two largest asset management firms in the world. Together with BlackRock, Vanguard has a hidden monopoly on global asset holdings and exerts control through their ownership of some 1,600 American companies.35
Combined, BlackRock and Vanguard own nearly 90% of all S&P 500 firms.36 To learn more about how Vanguard and BlackRock own just about everything in the world, and have monopoly control over all industries, check out the 45-minute video above, “Monopoly — Follow the Money.”
In short, the idea that there is competition in the marketplace is a cleverly disguised illusion. In reality, everything is controlled by a small group of asset managers that win no matter what. The end goal is to own and control all the world’s assets, which includes people.
The WEF slogan “You’ll Own Nothing and Be Happy” really summarizes The Great Reset plan for mankind. They will own everything; you will own nothing, not even your own body, and you’ll be too drugged up and lost in a make-believe computer game world to realize you’re a slave. If they can somehow make a profit from your useless existence, they’ll let you live. If they can’t, you’ll be eliminated. That’s really what the plan comes down to.
The plan for global authoritarianism is advancing with each passing day, but all is not lost yet. By informing ourselves and sharing what we know with others, we can reach the critical mass needed to end their plan and take back control.
It’s going to require standing together, unified in favor of freedom and liberty. It’s going to require legal and legislative efforts to weed out the corruption and infiltration that has occurred throughout the corporate world and our governments. It’s going to require honest men and women to step into positions of power that they never wanted. It may take a lot of time and effort, but if we want our descendants to experience freedom, no price can be too great to pay.
from Articles https://ift.tt/md92UA8
via IFTTT
Lifesaving Vitamin Slashes Heart Disease Risk by 57%
This article was previously published November 11, 2019, and has been updated with new information.
Vitamin K is a fat-soluble vitamin with significant health influence that many don't get enough of. Your body stores very little of it, so it's rapidly depleted without regular dietary intake. Common drugs can also deplete vitamin K, making elevated intake even more important.
There are many vitamin K-dependent proteins in your body, which are involved in things like blood coagulation, bone metabolism and mineralization of your blood vessels. As you'd suspect, that means vitamin K plays a particularly important role in the prevention of bleeding disorders, osteoporosis and heart disease.
There are two main forms of vitamin K, along with several subtypes, all of which can make matters a bit confusing. Here, I'll do my best to break down the basics, starting with the naturally-occurring forms of vitamin K and their basic functions and sources:1,2
1. Vitamin K1 (phylloquinone) — Vitamin K1 is derived from green, leafy vegetables such as spinach, kale, broccoli and cabbage, and is best known for the role it plays in blood clotting.
With insufficient K1, your blood cannot clot properly, which can have life-threatening consequences, as you could bleed to death. Excessive intake of dietary or supplemental K1 however, can overcome the anticoagulant effects of blood thinning medications.
As noted by vitamin K expert Leon Schurgers, Ph.D., absorption of vitamin K1 from food is low; only 10% of the vitamin K found in vegetables is absorbed, and there's no way to significantly increase that absorption.
2. Vitamin K2 (menaquinones) — The menaquinones play a primary role in bone and heart health. Inside your body, vitamin K2 is synthesized by certain bacteria in your gut. There are several subtypes of K2, two of the most common of which are:3
a. Menaquinone-4 (MK-4) — A short-chain form of vitamin K2 found in animal products such as meat, eggs, liver and dairy.4,5 Source matters, however. For example, pasteurized dairy and products from factory farmed animals are not high in MK-4 and should be avoided. Only grass fed animals (not grain fed) will develop naturally high levels.
MK-4 has a short biological half-life — about 2.5 hours — making it a poor candidate as a dietary supplement. That said, natural MK-4 from food is important for good health as it plays a role in gene expression. For example, research6 has found it may lower your risk of liver cancer.
b. Menaquinone-7 (MK-7) — Longer-chained vitamin K2 found in fermented foods such as sauerkraut, certain cheeses and natto.7 There's a variety of these long-chain forms, but the most common one is MK-7. This is the one you'll want to look for in supplements, as this form is extracted from real food, specifically natto,8 a fermented soy product.
MK-7 is produced by specific bacteria during the fermentation process. However, not all strains of bacteria make it,9 so not all fermented foods will provide it. Most commercial yogurts, for example, are virtually devoid of vitamin K2, and while certain types of cheeses, such as Gouda, Brie and Edam, are high in K2, others are not.
One of the best ways to ensure a good source of vitamin K2 is to ferment your own vegetables using a special starter culture with bacterial strains that produce vitamin K2. While K1 in vegetables is poorly absorbed, virtually all of the K2 in fermented foods is readily available to your body.
The MK-7 formed in the fermentation process has two major advantages: It stays in your body longer and has a longer half-life than MK-4,10 which means you can take it just once a day.
Research11 has shown MK-7 helps prevent inflammation by inhibiting proinflammatory markers that can cause autoimmune diseases like rheumatoid arthritis. And, while vitamin K1 has been found to moderately reduce the risk of bone fractures,12 MK-7 is more effective than vitamin K1 at reaching (and protecting) your bone.13,14
Vitamin K2 Plays Key Role in Heart Health
The difference between vitamins K1 and K2 was clearly established in The Rotterdam Study,15 published in 2004, which focused on their effects on the heart. As it turns out, K1 has no effect on the heart at all, whereas K2 does.
That doesn't mean K1 is useless — far from it. According to a 2019 study16 in the Journal of Gerontology, older individuals with low vitamin K1 status are more likely to have mobility problems and disability than those with higher levels. In reality, you need the whole suite of vitamin K, but vitamin K2 does have important benefits that K1 does not.
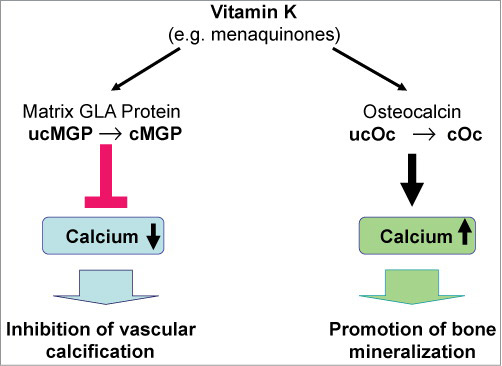
One of the reasons why vitamin K2 is so important for both bone and heart health in particular has to do with a complex biochemistry involving the enzymes matrix gla-protein (MGP, found in your vascular system17), and osteocalcin, found in your bone.
"Gla" stands for glutamic acid, which binds to calcium in the cells of your arterial wall and removes it from the lining of your blood vessels. Once removed from your blood vessel lining, vitamin K2 then facilitates the integration of that calcium into your bone matrix by handing it over to osteocalcin, which in turn helps "cement" the calcium in place inside your bone.
Vitamin K2 activates these two proteins, so without it, this transfer process of calcium from your arteries to your bone cannot occur, which raises your risk of arterial calcification.18
Calcium deposits in the arteries are responsible for atherosclerosis, hardening and narrowing of the arteries, slowly blocking blood flow. It's a common cause of heart attacks, strokes and peripheral vascular disease.
Indeed, studies19,20 have demonstrated vitamin K2 inhibits arterial calcification and improves arterial flexibility, thereby reducing your risk of a cardiovascular event (such as a heart attack) or death.21
One 2019 study22 proposed therapeutic supplementation with vitamin K2 could prevent or halt progression of vascular calcification that may occur with excessive calcium intake, and previous research has demonstrated those eating the highest amount of vitamin K2 have the lowest risk of developing cardiovascular disease.
In the Rotterdam study,23 those who had the highest amount of vitamin K2 were 52% less likely to experience severe calcification in their arteries and 57% less likely to die from heart disease over a seven- to 10-year period.
People who consumed 45 micrograms (mcg) of K2 daily lived on average seven years longer than people getting just 12 mcg per day. This was a profound discovery, because such a correlation did not exist for K1 intake.
In a subsequent trial called the Prospect Study,24 16,057 women were followed for an average of 8.1 years. Here, they found that each additional 10 mcg of K2 in the diet resulted in 9% fewer cardiac events. Again, vitamin K1 had no apparent impact on heart disease risk.
Vitamin K2 Is an Important Ally Against Osteoporosis
To explain the importance of vitamin K2 for bone health and prevention of osteoporosis a bit further, this goes back to its influence over osteocalcin.25 Osteocalcin is a protein produced by your osteoblasts (cells responsible for bone formation), and is utilized within the bone as an integral part of the bone-forming process.
However, osteocalcin must be "carboxylated" before it can be effective. Vitamin K functions as a cofactor for the enzyme that catalyzes the carboxylation of osteocalcin.
A systematic review and meta-analysis26 published in 2006 found vitamin K2, in this case MK-4, reduced bone loss and had "a strong effect on incident fractures." MK-4 supplementation was linked to a 60% reduction in vertebral fractures, a 77% reduction in hip fractures and an 81% lower risk for all nonvertebral fractures.
Another three-year-long placebo-controlled study27 done in the Netherlands found that postmenopausal women taking 180 mcg of MK-7 per day increased their bone strength, decreased the rate of age-related bone mineral decline and reduced bone density loss, compared to placebo.
Vitamin K2 'Kills Two Birds With One Stone'
Oftentimes, osteoporosis (precipitated by insufficient calcium in your bones) goes hand in hand with heart disease, and vitamin K2's interrelationship with MGP and osteocalcin is one of the reasons for that.
In short, both osteoporosis and heart disease are related to vitamin K2 deficiency, and can be prevented by ensuring sufficient amounts.
As noted in a 2015 paper,28 "By striking the right balance in intake of calcium and K2, it may be possible to fight osteoporosis and simultaneously prevent the calcification and stiffening of the arteries."
The following graphic from the 2014 paper,29 "Vitamin K: An Old Vitamin in a New Perspective," illustrates the effect of vitamin K on bone and vascular health.
Keep in mind that vitamin K2 also works in tandem with vitamin D and magnesium. So, it's important to remember that vitamin K2 needs to be considered in combination with calcium, vitamin D and magnesium, as these four all have a synergistic relationship that impacts your bone and heart health.30
Other Health Benefits of Vitamin K2
Vitamin K2 is also important for a variety of other health reasons and conditions, including the following:
|
Dental health — Preserving enamel helps reduce cavity formation. Your enamel is made of hollow tubes that extend into the dentin. The enamel is made of nonliving cells, while the dentin has live cells called odontoblasts. These cells release proteins using vitamin K2 to help prevent tooth decay through an immune response.31 Research32 has demonstrated osteocalcin may be found in inflamed tissue, and researchers consider the protein to have a reparative role in dental pulp. You teeth, like your bones, are storehouses of calcium, which supports the structure and hardness of the teeth.33 The way calcium is deposited in your teeth will either increase the hardness of your tooth or make it more brittle. Vitamin K2 once again acts like the traffic cop, telling calcium where and how to be used in your teeth. Working together with vitamin D, it also promotes a reduction in tooth decay or cavities.34 |
|
Cancer — Cancer prevention is another health benefit of vitamin K2. As noted in the 2010 European Prospective Investigation into Cancer and Nutrition (EPIC) study,35 high intake of vitamin K2 — not K1 — reduces cancer risk and lowers cancer mortality by 28%. Findings published in 2008 showed men who consumed the greatest amounts of K2 had a 63% reduced incidence of advanced prostate cancer.36 The evidence also suggests vitamin K2 may reduce your risk for Non-Hodgkin lymphoma. Mayo Clinic researchers discovered that people with the highest intake of vitamin K2 (108 mcg/day or higher) had a 45% lower risk for this type of cancer, compared to those with the lowest vitamin K2 intake (39 mcg/day or less).37 They attribute this effect to vitamin K2's ability to inhibit inflammatory cytokines, which are related to this type of lymphoma, and its role the life cycle of your cells. |
|
Inflammatory conditions — The inflammatory response is a crucial component in many chronic diseases and diseases of aging. Scientific evidence suggests both vitamin K1 and K2 have anti-inflammatory activity, in part by inhibiting nuclear factor kappa-B.38 In one meta-analysis,39 researchers found evidence the family of vitamin K plays a protective role in chronic aging conditions, inflammation and cardiovascular disease. Another study40 confirmed the role the MK-7 form specifically has in the modulation of inflammatory biomarkers. The researchers evaluated natural vitamin K2 for its potential to inhibit gene expression and production of pro-inflammatory markers in vitro, finding MK-7 inhibited gene expression in a dose-dependent manner. Other research41 has demonstrated a reduction in C-reactive protein, a common biomarker used to evaluate inflammation in patients with rheumatoid arthritis. C-reactive protein is a risk marker for a wide range of diseases and the researchers concluded higher intake of vitamin K2 may lower overall risk. |
|
Kidney health — There is also accumulating evidence suggesting vitamin K2 may play a role in chronic kidney disease. A pre- and post-intervention clinical trial,42 which included patients with a diagnosis of chronic kidney disease who took 360 mcg of MK-7 for four weeks, found it significantly reduced calcification in the patients' blood vessels. Patients with chronic kidney disease with a subclinical vitamin K deficiency may also benefit from a greater intake of the vitamin.43 As noted in a 2016 study44 in EBioMedicine, "MGP not only inhibits calcification in larger arteries but also may be renoprotective." |
|
Testosterone — Yet another role vitamin K2 plays in your body is the optimal production of sex hormones. At least two studies45,46 have shown MK-4, found in animal foods such as meat and dairy products, can help balance testosterone production. |
|
Polycystic ovarian syndrome (PCOS) — Vitamin K2 has an effect in women as well, as the vitamin may be helpful in the management of PCOS. This is now the most common hormonal disorders in young women, causing enlarged ovaries and a heightened risk for fertility problems.47 In one randomized study,48 60 vitamin D deficient women with PCOS took either a placebo or a combination of calcium, vitamin D and vitamin K for eight weeks. Those in the treatment group enjoyed greater decrease in testosterone and symptoms than the placebo group. |
|
Insulin sensitivity — An unexpected discovery was made when researchers found bone was an endocrine organ, contributing to the regulation of a number of physiological processes, including glucose homeostasis.49 There's evidence to suggest vitamin K2 supplementation may improve insulin sensitivity via osteocalcin metabolism,50 and may help prevent the development of Type 2 diabetes.51 The evidence is not conclusive, however, as a systematic review52 of controlled trials found K2 supplementation had no effect on insulin sensitivity. Part of the problem may have something to do with the form of vitamin given. Numerous studies have demonstrated synthetic vitamin K2 supplements are not as effective as natto-derived K2 supplements. |
|
Mitochondrial health — Research53 published in the journal Science in 2012 found vitamin K2 serves as a mitochondrial electron carrier, thereby helping maintain normal ATP production in mitochondrial dysfunction, such as that found in Parkinson's disease. |
|
Macular degeneration — According to a 2014 paper54 on vitamin K, MK-7 in particular may offer benefits for age-related macular degeneration. |
Signs and Symptoms of Vitamin K2 Deficiency
The major problem we face when it comes to optimizing vitamin K2 is that there's no easy way to screen or test for vitamin K2 sufficiency. Vitamin K2 cannot at present be measured directly, so it's measured through an indirect assessment of undercarboxylated osteocalcin. This test is still not commercially available, however.
Without testing, we're left with looking at various lifestyle factors that predispose you to deficiency. As a general rule, if you have osteoporosis, heart disease or diabetes, you're likely deficient in vitamin K2.
That said, it's believed that the vast majority of people are in fact deficient these days and would benefit from more K2. One reason for this is because very few (Americans in particular) eat enough vitamin K2-rich foods.
So, if you do not have any of the health conditions listed, but do not regularly eat high amounts of the following foods, then your likelihood of being vitamin K2 deficient is still very high:
- Certain fermented foods such as natto, or vegetables fermented using a starter culture of vitamin K2-producing bacteria
- Certain cheeses such as Brie and Gouda (these two are particularly high in K2)
- Grass fed organic animal products such as egg yolks, liver, butter and dairy
Use of certain drugs may also affect your vitamin K2 status and make you more prone to deficiency. For example, research55 shows statins deplete vitamin K2, and there's scientific evidence56 suggesting statin drugs may indeed increase calcification in the arteries.
Vitamin K2 depletion may be an explanation for that. So, if you're on a statin, you'll want to make sure you're taking extra vitamin K2, as well as ubiquinol or coenzyme Q10, which is also being depleted by the drug.
As discussed in "Vitamin K2 Deficiency Is a Significant Cause of Cardiovascular Disease," warfarin, antibiotics, anti-tuberculosis drugs, anticonvulsants can also raise your risk of vitamin K deficiency.
Dosage Recommendations
As for a clinically useful dosage of vitamin K2, some studies — including the Rotterdam study57 — have shown as little as 45 mcg per day may be sufficient. As a general guideline, I recommend getting around 150 mcg of vitamin K2 per day.
Others recommend slightly higher amounts; upward of 180 to 200 mcg. Fortunately, you don't need to worry about overdosing on K2, as it appears to be completely nontoxic.
If you opt for a vitamin K2 supplement, make sure it's MK-7. (The exception is if you're on vitamin K antagonists, i.e., drugs that reduce blood clotting by reducing the action of vitamin K. If so, you should avoid MK-7 supplements.58) Also remember to take it with fat since it's fat-soluble and won't be properly absorbed otherwise, and to balance it with calcium, vitamin D and magnesium.
As a last tip, keep in mind that vitamin K2 may not necessarily make you "feel better" per se. Its internal workings are such that you're not likely to feel the difference physically.
Compliance can therefore be a problem, as people are more likely to take something that has a noticeable effect. This may not happen with vitamin K2, but that certainly does not mean it's not doing anything.
from Articles https://ift.tt/KkBXcgS
via IFTTT
Eating Mistakes That Could Quietly Steal Your Later Years
This article was previously published February 24, 2019, and has been updated with new information.
Dr.Jason Fung, is a nephrologist and author of three books, "The Obesity Code," "The Complete Guide to Fasting," and "The Longevity Solution," which is the topic of this interview. This book was also co-written with James DiNicolantonio, Pharm. D, who also happens to be the co-author of my book, "Superfuel."
The motivation for "The Longevity Solution" came from a discussion with DiNicolantonio. "He'd already talked about salt in his book, 'The Salt Fix,'" Fung says. "In 'Superfuel,' he talked about good fats, bad fats and super fuel. We thought it would be great to tie everything together in terms of the real dietary determinants of longevity." Fung added:
"I spend a good section of the book talking about protein — the different types of protein, animal versus plant protein, for example, and how much protein [you need]. These are really important questions because there's so much [information] out there, and you don't know who to believe."
From my review of the book, I think that is probably one of the most valuable pieces, because there's so much confusion about protein. There's good reason for this confusion, because it's a complex topic. An important part of the equation is the mammalian target of rapamycin (mTOR), also known as the mechanistic target of rapamycin, a very important pathway responsible for controlling autophagy.
If you inhibit mTOR — which you can do by restricting protein — you activate autophagy, which is a good thing. However, I've personally made the mistake of not eating enough. While excess protein can activate mTOR, your protein needs do increase with age, as you need to counteract progressive loss of muscle mass. So, your age really needs to be taken into account as well.
Understanding the Role of mTOR
As noted by Fung, mTOR is basically a nutrient sensor. While insulin primarily senses your intake of carbohydrates, mTOR primarily senses protein. Different proteins will stimulate mTOR more than others. Fung explains:
"The reason is that mTOR senses the availability of protein and increases these growth pathways. If you're trying to increase muscle, like bodybuilders will, for example, then this might be a very good thing. On the other hand, it impacts aging. One of the real interesting theories of aging is that there's a sort of trade-off between the growth program and the longevity program.
That is, if you grow, it's actually the same pathway as aging. Whether it's good or bad depends on your age. When you're young, you want to grow, so you activate all these growth pathways. But as you get older, if you keep revving that growth engine, it's just going to burn out.
Just like your car engine, revving it is great if you want to go fast. But if, on the other hand, you want to keep that car for a long time, you don't want to rev it that much. Things change as you go along.
During childhood and early adulthood, you want that growth program to go forward, but that growth program is intrinsically at odds with the longevity program. After a certain point, you may want to cut things back. That's the understanding of mTOR; mTOR drives all this growth. But then as you get older, you wind up with diseases of too much growth …
There are all these chronic metabolic diseases where increasing the growth pathway, which is the same as the longevity-aging pathway, is not good. At some point, you want to slow it down. But as you get older, your body actually becomes resistant to some of these growth pathways.
Therefore, you actually need to take a little bit more. If you're elderly and you're at risk of falls, for example, then taking more protein might be a good thing. This is one of the reasons that protein is so hard to understand because everybody's so different … You just have to look at your own situation."
What Are Your Real Protein Needs?
All of that said, there are some general guidelines you can use to estimate your protein needs. Children, for example, generally need higher amounts of protein since they're in growth mode.
Now, when calculating your protein needs, it's important to make the calculation based on grams per kilograms (kg) of lean mass, not total body weight. The reason for this is because you do not need protein to maintain your fat mass. You need it to maintain your lean muscle mass. The following amounts can be used as a general guideline:
|
Children — 2 grams of protein per kg of lean body mass |
|
Young adults — 0.8 grams of protein per kg of lean body mass |
|
Adults — 0.6 to 0.8 grams of protein per kg of lean body mass |
|
Bodybuilders — 1 to 1.2 grams of protein per kg of lean body mass |
|
Endurance athletes — 1 to 1.5 grams of protein per kg of lean body mass |
|
Seniors — 0.8 grams of protein per kg of lean body mass; possibly more if muscle wasting is a problem |
The Importance of Cycling High and Low Protein Intake
The challenge here is find the balance so that the whole system is optimized. Muscle loss is a more or less inevitable consequence of age. But with age you also have more damaged cells that need to be removed by autophagy. My solution has been to devise a program in which I combine protein restriction with fasting, followed by increased protein intake on strength training days.
"I think that makes a lot of sense," Fung says. "If you look at the literature on longevity, the only really well-established thing that makes people live longer is calorie restriction, but it's very hard to do. One of the things is to cycle it back and forth, so that … some days, you're taking very little; some days you're taking a lot. I think that's actually how people were actually meant to live …
I think it makes a lot of sense because it's this sort of growth-versus-longevity paradigm. If you're always eating the same thing, then you're not going to be able to get that balance right. Because [when] you're in a pro-growth [pathway], that's also a pro-aging pathway.
You really want to go in between the two. Some days, you're going to take a lot. That will stimulate your mTOR, as well as insulin, for example, and put you in this growth pattern. Then you'll have days where your mTOR is going to be driven down very low. Those are the days your body's going to go into more of a survival mode, if you will. That's going to activate autophagy.
When you eat protein, for example, mTOR, which is a nutrient sensor, goes up. It basically just shuts off autophagy. Autophagy is this sort of cellular recycling process. It's very important for aging because it's a rejuvenating cycle for your cells …
When mTOR is very low, then your body will start to break down some of the subcellular parts. Those that are going to be broken down first are those older damaged parts. You're going to get rid of them all. Everybody thinks breaking down protein is bad. But it's not, because that's the first step in renewing yourself. You've got to get rid of all the old stuff and you've got to rebuild the new things. That's why it's important to cycle it …
I think you should, one day, maybe take 100 [grams of protein], and the next day zero. I think that's much better [than eating a specific amount of protein each day], because on the day you're taking zero, you get rid of all your old cells. Then on the day you're taking 100 grams, you're going to rebuild."
In addition to protein, other nutrients can also activate or inhibit mTOR:
- Nutrients that activate mTOR include branched-chain amino acids, glutamine, methyl folate and vitamin B12
- Nutrients thatinhibit mTOR include polyphenols like curcumin, fisetin quercetin, resveratrol (found in wine) and epigallocatechin gallate (EGCG, found in green tea). Organic coffee and dark chocolate also contain high amounts of mTOR inhibiting polyphenols
The Importance of Fasting for Longevity
In his book "Circadian Code: Lose Weight, Supercharge Your Energy and Sleep Well Every Night," Satchidananda Panda, Ph.D., cites research showing that 90% of people eat across 12 hours a day or more, and compressing this eating window may in fact be one of the most important things you can do for your health.
Fung recently published a case series paper1 detailing how fasting can be used as a therapeutic alternative for Type 2 diabetes. Three diabetic patients between the ages of 40 and 67 participated in a supervised fasting regimen to evaluate the effects on their insulin requirements. The patients had been diagnosed with Type 2 diabetes for 10, 20 and 25 years respectively, and were taking high doses of insulin daily.
Of the three patients, two did alternating-day 24-hour fasts, while one fasted for 24 hours three times a week over a period of several months. On fasting days, they were allowed to drink unlimited amounts of low-calorie fluids such as water, coffee, tea and bone broth, and to eat a low-calorie, low-carb dinner.
On nonfasting days, they were allowed both lunch and dinner, but all meals were low in sugar and refined carbohydrates throughout. (The complete manual of the fasting regimen used is described in Fung's book, "The Complete Guide to Fasting."2) Two of the patients were able to discontinue all of their diabetes medications while the third was able to discontinue three of his four drugs. All three also lost between 10 and 18% of their body weight.
"It was stunning because the time it took to get them off the insulin was between five and 18 days. The longest it took was 18 days … He had been told he'd be on it for the rest of his life … We got him off everything in 18 days," Fung says.
"We still follow those three … They're still off of all their medications. They manage it with their diet. The point is that if you have a disease that causes so much disability — Type 2 diabetes — you can allow your body to simply use up that excess sugar. It's like the body has too much sugar. That's the whole disease. Don't eat, and allow your body to burn it off. Now you have a completely free solution, a completely natural solution …
I don't know of anything that could be better for the treatment of Type 2 diabetes. It turns out there are all kinds of other benefits [as well] … Some of the research shows the average person is actually eating for 14 hours and 45 minutes per day. If you start eating breakfast at 8 a.m., you don't stop until 10:45 p.m. on average. This is the average American. That is unbelievable.
The point is [you need to] cycle. You have to put your body in a fed state. That is, you eat and your insulin goes up. Your mTOR goes up. But then you have to fast. There's a daily cycle that we're not respecting. There's a fed state. There's a fasted state … If you don't ever use that energy that you're putting into your body, you're just going to store it, and then it makes you sick."
Finding the Sweet Spot for Time-Restricted Feeding
Opinions about how long one should fast each day when intermittently fasting varies. Clearly, if your eating window is less than 12 hours, you're doing better than most. As a general rule, the recommended range is between 12 and 18 hours of fasting each day.
I'm of the opinion that 16 to 18 hours of fasting might be the sweet spot, as this allows your body to deplete the glycogen stores in your liver more and suppress mTOR and activate autophagy better. Fung agrees, saying:
"I think that somewhere around 12 to 14 hours is a sort of a baseline … The next step up is somewhere around 16 to 18 hours. That's so easy to do. Once you get used to it, it's so easy. You can build that right into your day without any problems at all. I think that's where you're exactly right. Your glycogen stores last about 24 hours.
But if you're following a lower carbohydrate diet, you're not going to build up those glycogen reserves. Therefore, in 16 to 18 hours, you're going to get down to that point.
Remember, when you've gotten rid of a lot of those glycogen reserves, then your body's going to go into this mode where you're going into gluconeogenesis, which is starting to break some of the proteins down, which everybody thinks is bad, but I actually think is a highly beneficial thing, because you will rebuild that.
Then you start to get into burning fat. That's really where you want to be on a daily basis, 16 to 18 [hours of fasting]. It allows you to just jump into the 20- to 24-hour [fasting] range without any difficulty if you're at that baseline already."
How Growth Hormone Is Affected by Fasting
Many hormonal shifts occur during fasting. Paradoxically, growth hormone, which would appear to stimulate mTOR, does increase when you fast — increasing two to three times its baseline level within 24 hours of fasting — yet mTOR is suppressed during fasting. Fung explains:
"The growth hormone question is really interesting, because it does seem paradoxical. Why would your body make all this growth hormone if you've got nothing to eat? It's because the growth hormone acts through the liver to produce insulin-like growth factor 1 (IGF-1) … which mediates all the effects of growth hormone. If you knock out IGF-1 and give growth hormone, it has no effect.
During fasting and calorie restriction as well, your liver downregulates the growth hormone receptor in the liver. So [while] the growth hormone level goes way up, your body's not that receptive to it. Therefore, there's not a lot of IGF-1 going on. That's very interesting.
Because then when you eat again, this is when that big surge of growth hormone can start to hit you, and then you can start to rebuild all your muscle and so on … That's, again, is [part of] this rejuvenation process and this antiaging process."
Since your growth hormone level will remain elevated for up to 48 hours, you can further optimize your fitness by doing strength training on the day you break your fast, as then you will enter your workout with a very high growth hormone level, allowing for maximum muscle growth.
"That's what people do [when] training in the fasted state. They fast for 18 to 24 hours, get the high growth hormone levels, train and then they eat. That's when you got the big growth hormone surge. What they found also was that when you exercise, your body becomes more responsive to this growth, of course, because it wants to rebuild. But it'll last for like48 hours," Fung says.
"You don't have to eat before you exercise. You can exercise, then anytime within the next 24 to 48 hours, if you eat a lot of protein or whatever, you're going to have that rebuilding, because the growth hormone is there. The body is in that state where it's trying to rebuild."
One slight caution here is that fasting, being a stressor just like exercise, will also increase the stress hormone cortisol. While for most people, exposure to this mild stress every day will make them stronger and healthier, for some it may be problematic, and may require you to tweak your fasting schedule. You may find your body responds better to a once-a-week 24-hour fast, for example, opposed to daily intermittent fasting.
More Information
Fung also discusses the benefits of tea, known for their longevity-boosting effects. Green tea is rich in catechins such as ECGC. Fung likes Pique Tea Crystals, which contain far higher amounts of catechins than regular green tea. Just remember, for tea to be beneficial, you need to drink it "straight," without sweeteners and milk.
Whole leaf teas will also typically be of higher quality than bagged teas. Black tea contains thioflavins, which also appear highly beneficial. "Tea, I think, is one of the underappreciated sorts of things. I think it's just a part of a healthy lifestyle," Fung says, adding:
"The book itself, I think, is fantastic. It goes through everything sort of in a shorter form. If you want to get more information on fasting, you can go to 'The Complete Guide to Fasting.' If you want to get more information on salt, you can go to James' book, 'The Salt Fix.' If you want to get more information about healthy fats, you can go to 'Superfuel' or 'Fat for Fuel' … ['The Longevity Solution'] is sort of a synthesis of all that.
Then what we do is we look at the blue zones, which is these long-lived populations, and … see how they stack up [against] these simple ideas that we put out there for healthy living.
We also looked at this very interesting study called the 'Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma' (REGARD), which looked at the Southern diet, which is of the southern United States.
Turns out that fad diet is highly, highly detrimental. Why? It's a lot of processed foods, a lot of processed meats, processed fats, high in salt but not good because it's all processed …"
If you're intrigued by what you've heard so far and want to learn more, be sure to pick up a copy of "The Longevity Solution." In addition, my book, "Ketofast" is also available.
  >>>>> Click Here <<<<< |
 >>>>> Click Here <<<<< |
from Articles https://ift.tt/ZsdhfAl
via IFTTT
Hyperbaric Therapy — A Vastly Underused Treatment Modality
Dr. Jason Sonners, author of the book, “Oxygen Under Pressure: Using Hyperbaric Oxygen to Restore Health, Reduce Inflammation, Reverse Aging and Revolutionize Health Care,” started out as a chiropractor. His passion, however, is hyperbaric oxygen therapy (HBOT), which is the focus of his Ph.D. studies at the University of Miami.
While commonly used to speed up stubborn wounds and tissue infections, hyperbaric medicine can also be helpful in the treatment of infectious diseases such as COVID. It’s also enormously useful for stroke patients. I can't think of a more effective intervention than to get the stroke patient into a series of hyperbaric treatments as quickly as possible.
HBOT for General Health and Disease Reversal
Every cell in your body, with the exception of your red blood cells (which have no mitochondria that require oxygen), requires oxygen to create energy. Many chronic diseases of the modern world involve decreased mitochondrial function, increased systemic inflammation, and an inability of cells to generate the required amounts of energy for optimal function.
“We use hyperbaric oxygen, traditionally, for these terrible and severe conditions,” Sonners says. Unfortunately, it’s typically a last resort, literally right before an amputation surgery or as a life-saving mechanism for somebody with carbon monoxide poison or air gas embolism.
“So, we only think about it, traditionally, to help save the life or limb of somebody in a really severe condition, but the mechanisms that are working for those folks are very similar to the reasons that you and I might consider using hyperbaric oxygen:
For upregulating the oxygen levels inside your body, which will help reduce inflammation, increase mitochondrial function ... and thereby increasing the energy that those cells are able to generate ...”
HBOT for Chronic Diseases
Sonners’ goal is to expand the use of HBOT from the acutely life-threatening issues like gangrene to more chronic conditions, such as autoimmune and neurodegenerative diseases.
“My thought process is that the mechanisms of action of hyperbaric are the same whether we're talking about gangrene, radiation burns and osteonecrosis, or TBI [traumatic brain injury], concussion, maybe MS [multiple sclerosis] and post-stroke.
If we really get a mastery of the mechanisms of action, we can start to apply those mechanisms across the board. Clinically, we've seen hyperbaric work for so many of these other chronic illnesses ...
So, if we could really home in on those mechanisms and understand them better, and then get a better feeling for what time and pressure settings we require in order to get those mechanisms to kick in, then we can really, with more confidence, apply this therapy to these other conditions and have more consistent results in doing so.
A lot of the work I'm proposing to do is tagging onto some of this work in regenerative medicine, where they were looking at the collagen, fibroblast and stem cell response to hyperbaric. A study came out in 2020 on telomeres, and looking at this potential, upwards of 20% increase in telomere length, especially in certain immune system cells.
I want to build on that knowledge base, so what I'm doing is I'm creating a study that's going to have a lower-pressure group and a higher-pressure group, and we're going to be looking at a whole cytokine panel, so we can understand the mechanisms of the anti-inflammatory side.
We're going to have a methylation panel so that we can start looking at the epigenetic effects of hyperbaric. We're going to have a telomere component, similar to the telomere study that was done a year and a half ago.
And we're going to start comparing all of those metrics across roughly a three- to six-month timeframe of treatment, and over two separate pressure settings, to better understand which pressures are getting which effects, and again, what period of time should we be expecting before we get the results that we're looking for?”
Research Underway
On the low end, Sonners will be using 1.3 atmospheres (4.2 PSI) at 100% oxygen, and on the high end, he’ll use 2.0 atmospheres (14.7 PSI) at 100% oxygen. All patients will use hard chambers at two different pressures. The lower pressure group will be at 4.2 psi, which is the same as soft chamber pressures.
“There's nowhere near the amount of research in soft chambers as there are in hard chambers,” Sonners says. “The overwhelming majority of research is done at that 2-atmosphere range, which is why I'm choosing that as the upper end of the research that I'm doing in the soft chamber research.
There is definitely some [research] on sports recovery. There's actually some ongoing studies right now on hyperbaric for stem cell use that we're waiting for. In some cases, 1.3 [atmospheres] has been used as the sham group, opposed to a treatment arm in the research. Maybe the study team really thought that 1.3 wasn't going to have an effect and it's a legitimate sham ...
I'm not sure, but there are some great studies. There's a study that was done on cerebral palsy (CP) and 1.3 was used as the sham group ... In this particular study, with 1.3 being the sham group, there was also a ... control group that got no hyperbaric at all.
Within the sham group, there was significant improvement on the metrics they were measuring. Then they had a 1.5 [atmospheres at] 100% oxygen, which also had a good improvement and then, a 1.75 [atmospheres at] 100% oxygen, which had even a greater improvement.
The issue in the study was that while all three of those groups improved, there was no statistical difference or enough of a statistical difference between the 1.3, the 1.5 and the 1.75. So, the conclusion of the study was therefore that hyperbaric does not work for CP, although all three of those groups had significant improvement.
So, because the sham group was not considered a treatment, that was the conclusion of that study. Now, the natural consequence of that should have been redoing the study and creating a different level of what the sham and the treatment arms ought to be, but that was never redone.
So, as a result, there's this study with results that say hyperbaric does not work for CP. Meanwhile, clearly, what it means is we need more studies. It's just that studies are expensive. They’re very time consuming and you really have to have a large interest in trying to come up with the right answers to put forth the effort and time and money to get that kind of work done.”
Mechanisms of Action
If you breathe 100% oxygen under pressure, it’s intuitively obvious that you're going to deliver more oxygen to your tissues. That’s one clear mechanism, but it’s not the only or even primary reason for most of the benefits of hyperbaric therapy.
Evidence suggests part of the benefit might be related to the degeneration of a molecule called hypoxia-inducible factor alpha (HIF-1 alpha), which is generated when you lower the pressure. The pressure is high inside the chamber, and is lowered when you exit the chamber and enter the normal atmosphere. That means some of the benefit might actually be occurring when you get out of the chamber. Sonners explains:
“We don't have an exact number right now, but roughly half of the treatment is occurring while you're in the chamber, being exposed to the pressure, being exposed to the oxygen and literally accumulating a surplus of oxygen because of the therapy itself.
The other half of the therapy is when you get out of the chamber, as that oxygen can no longer stay in solution. It literally starts trying to bubble out of solution. As that happens, it's not inert, it's actually very active. So, as it's coming out of solution, it's interacting with all of our cells.
As a result, it's triggering a massive cascade of events, cellular communication that seems to stimulate multiple series of regeneration and anti-inflammatory [events], even within the reactive oxygen species themselves.
When we look at the first part, which is the dosage of oxygen a person is getting, and that's measurable, you could say, ‘Here's a person, they were in a chamber, they were at this pressure, breathing this percentage of oxygen for this amount of time,’ and you could literally calculate the theoretical dose of oxygen that person was exposed to and should have been able to absorb.
We've kind of just stayed in that mindset for all these years. [However], there was a great paper out of Israel called ‘The Hypoxia-Hyperoxia Paradox,’ and what they're saying is we know that there's amazing benefits of hypoxia actually.”
Benefits of Relative Hypoxia
Some of these benefits include the stimulation of HIF-1 alpha, stem cell responses, collagen responses and the angiogenic responses. For these reasons, Sonners views hyperbaric as an anabolic therapy — a therapy that stimulates vitally important growth and repair, as growth factors such as VEGF (vascular endothelial growth factor), and BDNF (brain derived neurotropic factor) are both stimulated.
Again, these growth factors are not stimulated by the hyper-oxygenation. They're a result from the hypoxic component, the process your body goes through as the oxygen is leaving your body.
“The important thing to note is that once you've accumulated all this extra oxygen, your hyper-oxygenation component, as that oxygen is leaving your body, you're never truly hypoxic,” Sonners says, “but the cell signaling factors that respond to traditional hypoxia are also seemingly responding to this relative hypoxia.
If you look at that paper [‘The Hypoxia-Hyperoxia Paradox’] ... it seemed to delineate this. With hypoxia alone, you will still get VEGF, which means you'll still get a lot of angiogenics, the rebuilding of the endothelial lining, the creation of a new micro-circulation bed, all this capillary regrowth will happen from hypoxia.
You'll get these stem cell releases, this potential for increase in the regenerative nature of cells. You'll get this increase in the HIF-1 alpha. But if you're chronically hypoxic, you're also going to get a downregulation of sirtuins [longevity proteins] and you're going to get a downregulation of mitochondrial function.
Sirtuins could play a great role in things like cell cycle life, getting cells out of cellular senescence — kicking them back into active life — or apoptosis, killing that cell so that we can replace it with a new stem cell, or even the genetic and epigenetic repair mechanisms. A lot of that has to do with sirtuins, so we don't want to downregulate those. We want to upregulate those.”
So, to clarify, with HBOT, you get the benefits of hypoxia with none of the downsides. Rather than inhibiting sirtuins, which are important for health and longevity, you actually get an upregulation of sirtuin activity. It also upregulates mitochondrial function and boosts mitochondrial replication, which the complete opposite to what happens in true hypoxia.
What About the Free Radical Component?
Without any doubt, HBOT is a type of oxidative stress, but it doesn’t have the adverse effects you’d expect. Sonners explains:
“There was a great paper done by Dominic D'Agostino and Angela Poff, back in 2017 or 2018, specifically looking at the reactive oxygen species or the free radical component of hyperbaric oxygen. What are the benefits or consequences as we upregulate, as we increase the amount of oxygen into the body?
As the cells and the mitochondria start to uptake that oxygen, producing more energy, there is a natural consequence where this byproduct of free radicals are released as a part of normal cellular respiration. Excess free radicals is obviously consequential to cell membranes, lipid peroxidation and protein degradation.
It could destroy cell membranes, mitochondrial membranes, nuclear membranes, genetic material ... At the same time, it's a normal response to cellular respiration and our bodies have their own intrinsic mechanisms for dealing with some of this excess free radical, things like the superoxide dismutase, catalase and glutathione pathways.
So, there seems to be a distinction that we should make. One is that some of the free radicals our bodies are exposed to come from the outside world in. Radiation, smoking, air pollution, the list goes on and on. So, we need to have a robust, intrinsic ability to tolerate these free radicals with our own antioxidant system.
But in excess, we could be getting too much free radicals and we could be depleting our own systems, in which case supplementation should certainly be considered and used. On the flip side, we look at hyperbaric oxygen as this tool that theoretically has all these great effects, but one of those consequences would also be this increase in free radical exposure.
There seems to be a very big delineation between a body that's exposed to free radicals from the outside world, versus a body that is exposed to free radicals that it's creating on its own.
One of those distinctions is that through the use of hyperbaric oxygen, even without supplementation, and the increase in free radical production from mitochondrial ATB production, the body itself — assuming it has the right raw materials — will actually increase its own superoxide dismutase, catalase and glutathione pathways.
This would No. 1, help make you more resilient to hyperbaric oxygen, but No. 2, would also help make you more resilient to all the other free radicals that you’re potentially exposed to in your environment.
So, I would say two things. One, especially with patients who are a little bit more fragile when it comes to oxidative stress, those people, I would tend to not over oxidize to begin with, so I might start at a gentler hyperbaric protocol with them, and I'm likely to want to start quickly upregulating their own system, getting the right supplementation for improving their intrinsic antioxidant systems ...
Then, as their system improves their tolerance for reactive oxygen species, we may not need as much of that, or if we're going to be using high dose hyperbaric oxygen for a period of time, we might use things like certain SOD precursors, or molecular hydrogen.
Through conversations with you, it has become one my favorite antioxidants that we use. Between 45 minutes to an hour before [hyperbaric treatment], we’ll start loading people with the molecular hydrogen as a mechanism to reduce the consequences. There are benefits, in other words. Reactive oxygen species on its own also helps stimulate hormone balance and helps stimulate cell repair by themselves. So, there has to be this balance.
We don't want to quelch all the free radicals because free radicals are a very important signaling molecule for so much cellular activity and at the same time, we want to be aware of the fact that hyperbaric does increase that, and we want to make sure that we're not over-exposing somebody.”
HBOT Functional Medicine Course Now Available
Sonners also reviews the curriculum he developed for the International Board of Undersea Medicine. The IBUM has been certifying people in hyperbaric medicine for 25 years, and the curriculum Sonners created has been taught as a functional medicine hyperbaric course for clinicians for the past year.
“A big push for me, and even for the research I'm doing, is to help create awareness that gets more doctors excited about [HBOT], that want to actually use it in their practice,” Sonners says. “So, this has been an attempt to really improve the education so that people aren't just going to hyperbaric courses to learn about wound care.
We needed courses to help practitioners like myself or other people interested in the regenerative side to be able to learn how to apply it that way. So, we now have a course that I teach a few times a year to get people on the same page.
The majority of this last year, other than getting through school and writing the thesis, has been developing and promoting that course. I think we've certified about 125 to 150 practitioners and technicians specifically on the functional medicine side of hyperbaric use ...
At this time, I still see a pretty big mix between soft chamber use and hard chamber use. A lot of those doctors are either Dos, MDs, chiropractors or naturopaths, getting into more of a functional medicine base, just looking for other natural approaches to the things they are treating.
Hyperbaric supplies the body with a fundamental ingredient and it's so necessary for cellular performance. It just seems to make sense to start implementing a tool and a modality like that into a setting where you're trying to reduce inflammation, you're trying to improve energy production cellularly.”
HBOT Has at Least 100 Indications for Use
While the list of potential uses for HBOT is extremely long, in the U.S., the Food and Drug Administration has approved and most insurance will pay for HBOT for the following 14 conditions:1
|
Air or gas embolism |
Carbon monoxide poisoning |
|
Clostridial myositis and myonecrosis (gas gangrene) |
Crush injuries, compartment syndrome and other acute traumatic ischemia |
|
Decompression sickness |
Arterial insufficiencies, such as central retinal artery occlusion |
|
Severe anemia |
Intracranial abscess |
|
Necrotizing soft tissue infections |
Osteomyelitis |
|
Delayed radiation injury (soft tissue and bone necrosis) |
Compromised grafts and flaps |
|
Acute thermal burn injury |
Idiopathic sudden sensorineural hearing loss |
In terms of conditions that can benefit from HBOT, I would certainly add stroke, TBI, heart attack, anytime there's post ischemic reperfusion injury, and most neurodegenerative conditions. Internationally, there are about 100 recognized indications. While that might make it sound like a magical cure-all, it’s important to remember that it doesn’t cure anything directly.
What it does is provide your body with a foundational nutrient, oxygen, that virtually all cells require. HBOT supplies your body oxygen in a surplus, creating an excess reservoir of oxygen to improve that function. That’s why it can help improve such a wide variety of health conditions.
Even autoimmune diseases such as MS, lupus and rheumatoid arthritis, just to name a few, may benefit, Sonners says. A whole other category of potential use would be wellness, longevity and regenerative-type therapies.
“We're just applying the tools slightly differently to help match the intensity of the therapy to the severity of the condition. We can utilize the principles of gas exchange in various ways to help so many different types and various types of conditions,” Sonners says.
“One condition or subclass that we talked about it in the beginning is, from the immune system standpoint, upregulating your ability to fight infection by increasing white blood cell activation through the reactive oxygen species mechanisms. We use it for anaerobic infection, bacterial infections all the time.
One of the main reasons that hyperbaric works in those severe conditions is those bacteria are anaerobic. They don't live in high oxygen environments.
So, we know that putting a patient in a high oxygen environment massively decreases bacteria's ability to function, potentially helps to kill that infection, helps to block the toxicity of that infection and helps to break down the biofilms around that infection. So, hyperbaric becomes an amazing tool in the capacity of immune system balancing and/or ability to help fight infection.”
More Information
As a general guidance, Sonners recommends doing hyperbaric for about two hours a week on a regular basis. That’s his personal routine. In addition to that, three times a year he does a 30- to 40-hour protocol over the course of six to eight weeks. He explains why:
“We know that in general ... three or four sessions is not going to ever cut it. The main effect of hyperbaric is really achieved through the cumulative effect and the increasing and decreasing — the wave of hyper-oxygenation back to normal oxygen levels — creating that hyperoxia-hypoxia type paradox ...
When you do a protocol similar to like what I would do for a patient, let's say four to six hours a week for eight weeks, the frequency of those ... the space in between them, really shrinks and you get far more signaling to occur ...
If all we cared about was the physical dose, we would stay at 100% oxygen as long as we possibly could, at the highest pressure we could tolerate to get the most oxygen absorption. I don't think that that's where the majority of benefit exists.
Every time your pressure changes or your percentage of oxygen changes, you're stimulating HIF-1 alpha, the reactive oxygen species load, sirtuins, you're signaling a hormetic effect. I picture them as switches. You're flipping that switch on, off, on, off, on, off. I think it's the amount of times that you stimulate that switch that will create the benefits we're looking for, more than the physical dose of oxygen over time.”
To learn more about HBOT in general, be sure to pick up Sonners’ book, “Oxygen Under Pressure: Using Hyperbaric Oxygen to Restore Health, Reduce Inflammation, Reverse Aging and Revolutionize Health Care.”
In the interview, we also discuss how you can incorporate HBOT in your fitness routine, along with fasting, to augment and upregulate cellular performance, recovery and regeneration. So, if that’s of interest to you, be sure to listen to the interview in its entirety, or read through the transcript.
from Articles https://ift.tt/2ibsNZ8
via IFTTT
MKRdezign
Powered by Blogger.