Health, Fitness,Dite plan, health tips,athletic club,crunch fitness,fitness studio,lose weight,fitness world,mens health,aerobic,personal trainer,lifetime fitness,nutrition,workout,fitness first,weight loss,how to lose weight,exercise,24 hour fitness,
Labels
Technology
New Post
[recent][newsticker]
May 2020
Top Health News -- ScienceDaily
Aging
Alzheimer's
Articles
Articles : Asthma
Articles : CAFO
Articles : Children's Health
Articles : Cholesterol
Articles : Emotional Health
Articles : Fibromyalgia
Articles : GMO
Articles : Heart Health
Articles : Hormones
Articles : Internal Videos
Articles : Interviews
Articles : Men's Health
Articles : Politics
Articles : Thyroid Disease
Articles : Vaccines
Autism
best natural health source
Children's Health
Detoxification
Diabetes
Diet | body+soul
Diet and Weight Loss News -- ScienceDaily
Digestive Diseases
Dite
Dite & weight loss
Drug Industry
Drugs
EFT
EMF
Emotional Health
Finances
fitness
Fitness | body+soul
Fitness/Exercise
Fluoride
Food
Fructose/Sugar
Gardening
Harvard Health Blog
Health
Health | body+soul
Health and Wellness
health news
health tips
Heart Health
information
Joint Support
Juicing
Men's Health
news
Nutrition
Nutrition | body+soul
Pollution
Raw Milk
Soy
Supplements
Swine Flu
Technology
Thyroid Disease
Top Health
Top Health News -- ScienceDaily
Under Armour
Vaccines
Weight Management
women's health
Women's Health News -- ScienceDaily
work place health
Workplace Health News -- ScienceDaily
The Vitamin D Level to Reach Before Second Wave of COVID-19
As reviewed in “Vitamin D Level Is Directly Correlated to COVID-19 Outcomes,” there’s compelling evidence to suggest optimizing your vitamin D level can reduce your risk of COVID-19 and other viral infections such as seasonal influenza.
A number of different scientists are calling for people and governments to prepare for a second wave of COVID-19 come fall, both in the U.S. and abroad.1 Considering SARS-CoV-2 has been shown to be responsive to temperature and humidity, with infectiousness increasing with lower temperatures and humidity levels, we’re likely going to see a reemergence of COVID-19 infections in the fall, during normal influenza season.
REALLY IMPORTANT: Optimize Your Vitamin D Level Before Fall!
What this means is you now have a known “deadline” for optimizing your vitamin D level. To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 nanograms per milliliter (ng/mL) and 80 ng/mL by fall. In Europe, the measurements you’re looking for are 150 nanomoles per liter (nmol/L) and 200 nmol/L.
Historically, December typically has highest flu activity in the U.S.,2 but it would probably be good to aim for October, or maybe even earlier depending on your location. Optimizing your vitamin D is particularly important if you have darker skin, as darker skin places you at higher risk for vitamin D deficiency — and serious COVID-19 infection.
COVID-19 Racial Disparity Rooted in Vitamin D Deficiency
As reported by The Guardian,3 the COVID-19 mortality among black Americans is three times higher than that of whites, and researchers have long known that blacks cannot achieve optimal vitamin D levels from sun exposure at any time of the year in Northern America.4
Research5 posted April 28, 2020, points out that vitamin D insufficiency is prevalent in severe COVID-19 cases and that “Emerging health disparities data regarding African-American and homeless populations suggest that vitamin D insufficiency (VDI) may be an underlying driver of COVID-19 severity.” Importantly, this study6 found 100% of COVID-19 patients under the age of 75 admitted to intensive care units had vitamin D insufficiency.
A letter to the editor,7 published in the Irish Medical Journal, also points out the many links between vitamin D deficiency and factors known to play a role in COVID-19, such as male sex, acute respiratory distress syndrome (ARDS) and comorbidities like obesity, diabetes and heart disease, and presents data from an in-hospital review of 33 male COVID-19 patients’ vitamin D levels.
The 12 patients who progressed to ARDS had a mean vitamin D level of 27 nmol/L (10.8 ng/mL), whereas those who did not progress to ARDS had a mean level of 41 nmol/L (16.4 ng/mL).
It’s worth noting that 16.4 ng/mL is still grossly insufficient, as 40 ng/mL (100 nmol/L) has been established as a minimum level of sufficiency for general health and disease prevention by GrassrootsHealth.8 The same goes for the elderly, as you tend to lose the ability to convert vitamin D from sun exposure as you age.
Step 1: Measure Your Vitamin D
So, how do you go about optimizing your vitamin D level? First, you need to find out what your base level is, which is done using a simple blood test. An easy and cost-effective way of doing this is to order GrassrootsHealth’s vitamin D testing kit.
Once you know what your blood level is, you can assess the dose needed to maintain or improve your level. Again, the ideal level you’re looking for is above 40 ng/mL, and ideally between 60 ng/mL and 80 ng/mL (European measurement: 100 nmol/L or, ideally, 150 nmol/L to 200 nmol/L).
The easiest way to raise your level is by getting regular, safe sun exposure, but if you’re very dark-skinned, you may need to spend about 1.5 hours a day in the sun to have any noticeable effect.
Those with very light skin may only need 15 minutes a day, which is far easier to achieve. Still, they too will typically struggle to maintain ideal levels during the winter. So, depending on your situation, you may need to use an oral vitamin D3 supplement. The next question then becomes, how much do you need?
Step 2: Assess Your Individualized Vitamin D3 Dosage
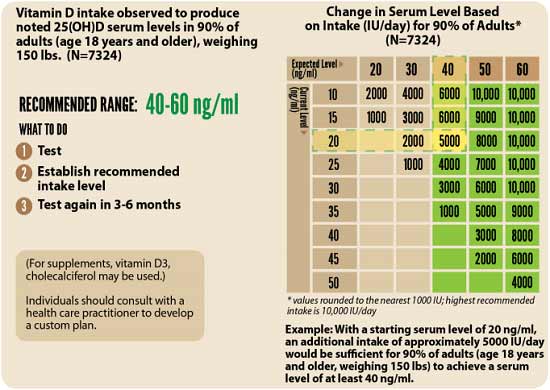
The reason you do not want to get fixated on arbitrary dosage recommendations is because the required dose can vary greatly depending on several factors, including skin color, weight and other nutritional deficiencies. As explained by GrassrootsHealth:9
“One of the main factors contributing to this variability is a person’s weight. Therefore, we also calculated a dose-response curve adjusted to an individual weighing 150 pounds (68 kg), shown below.
Indicated on the chart are supplemental dose amounts that ensure a specific proportion of the population achieves particular vitamin D levels. For example, 55% of participants achieved at least 40 ng/ml with 2000 IU/day and 94% of participants achieved at least 40 ng/ml with 8000 IU/day. This chart can be used as a guide to select your starting dose.”

While this chart provides a starting point, you can fine-tune your dosage further by taking into account your baseline vitamin D level. To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. To convert ng/mL into the European measurement (nmol/L), simply multiply the ng/mL measurement by 2.5.
How to Calculate Your Vitamin D From Sun Exposure
To calculate how much vitamin D you may be getting from regular sun exposure in addition to your supplemental intake, consider using the DMinder app,10 created by Dr. Michael Holick, author of “The Vitamin D Solution: A Three-Step Strategy to Cure Our Most Common Health Problems.” The free app is available for iPhone and android in the Apple store and Google play respectively. As explained by imedicalapps.com:11
“The app attempts to calculate a patients’ vitamin D level based on demographics imputed when first opening the app and then updates the level based on either actual lab draws or data from the app. The app even uses the phone’s GPS and clock to determine the ‘best’ time of day for a patient to get the required sun exposure for vitamin D skin conversion.”
Step 3: Retest
Next, you’ll need to re-measure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you. As explained by GrassrootsHealth:
“The only way to know how much supplemental intake you need is to test your levels. This will tell you whether the dose you are taking is the right dose for you to reach optimum nutrient levels. It is also important to check your nutrient levels at regular intervals because lifestyle changes may create a need for dosing adjustments.”
What Is the D*action Project?
Aside from the DMinder app, another helpful tool is the myData-myAnswers online tracker created by GrassrootsHealth. You automatically have access to this tool when you buy their vitamin D testing kit and enroll in the D*action project.
You can track any given supplement with this tracker (not just vitamin D). By tracking exactly how much you take and when, you can get a clearer picture of your personal requirement to reach and maintain an ideal level.
When you buy the GrassrootsHealth testing kit, you agree to enroll in the D*action project, an international field study aimed at solving the vitamin D deficiency epidemic.
By sharing your test results and anonymized personal health data with GrassrootsHealth researchers, you will enable them to determine the details of how vitamin D impacts health. As explained by GrassrootsHealth:
“You may choose to enroll 1-time to test your levels with an extended health questionnaire or you may participate for the full 5-year project where you provide your health information each 6 months for the 5-year period. The participation fees are based on the tests chosen; additional tests can be added to fit your individual needs.”
While I make these testing kits available in my online store, I do not make any profit from their sale. All proceeds go directly to GrassrootsHealth. If you prefer, you can also obtain the kit directly from their website.
Share and Inform Your Community
I urge everyone to share this information with friends, family and community at large, so that we can minimize a second outbreak. For example, you could speak to pastors in churches with large congregations of people of color and help them start a program getting people on vitamin D. Doing so could help save many lives; far more than any vaccine program.
Additionally, if you have a family member or know anyone that is an assisted living facility, you could meet with the director of the program and encourage them to get everyone tested or at least start them on vitamin D.
from Articles https://ift.tt/2XjSdlo
via IFTTT
Weekly Health Quiz: Stress, COVID-19 and Bill Gates
1 Which of the following may be a beneficial adjunct in COVID-19 treatment by reducing oxidative stress, counteracting hypercoagulation and breaking down blood clots?
- Hydroxychloroquine
- N-acetylcysteine (NAC)
NAC may be a useful adjunct in COVID-19 treatment due to its ability to reduce oxidative stress, counteract hypercoagulation and break down blood clots. Learn more.
- Fish oil (omega-3)
- Vitamin D
2 What sets SARS-CoV-2 apart from other known coronaviruses?
- It's human RNA
- It's ability to infect both animals and humans equally
- It's unique spike protein
What sets SARS-CoV-2 apart from other known coronaviruses is its unique spike protein that allows it to infect human cells. Learn more.
- It's inability to infect animals
3 Which of the following is currently the largest funder of the World Health Organization?
- Eric Schmidt
- The United States
- The United Kingdom
- Bill Gates
As the U.S. has halted funding of the WHO, Bill Gates has become the largest funder of this global health organization. Learn more.
4 Which of the following has been shown to impact your risk of testing positive for SARS-CoV-2, illness severity, and COVID-19 mortality?
- Vitamin D status
Vitamin D concentrations are lower in patients with positive PCR (polymerase chain reaction) tests for SARS-CoV-2, and countries with lower vitamin D levels have higher mortality rates from COVID-19. Recent research also shows vitamin D levels are strongly correlated to the severity of the illness experienced. Learn more.
- Prophylactic hydroxychloroquine use
- Quercetin supplementation
- Mineral status
5 Which of the following doctors has developed two effective treatments involving vitamin C and steroids, one for the treatment of sepsis and another for COVID-19?
- Dr. Mehmet Oz
- Dr. Paul Marik
Dr. Paul Marik has developed two effective treatments involving vitamin C and steroids, one for the treatment of sepsis and another for COVID-19. Learn more.
- Dr. Sanjay Gupta
- Dr. Kevin Pho
6 Genetic data suggests SARS-CoV-2 is a:
- Naturally evolved virus that jumped from animal to human
- Fabricated virus that does not exist in the real world
- Laboratory altered virus
Genetic data suggests SARS-CoV-2 is a laboratory created virus. Learn more.
- Naturally evolved virus incapable of infecting humans
7 Which of the following can significantly increase your risk of serious COVID-19 infection?
- Vaccine deficiency
- CBD oil use
- Being younger than 20
- Vitamin D deficiency
Recent studies suggest vitamin D deficiency significantly increases your risk of serious illness and death. Learn more.
from Articles https://ift.tt/3cnflE6
via IFTTT
Nourish Mint — A Plan for Farmers and Natural Businesses
The unemployment caused by the coronavirus pandemic will soon exceed that of the Great Recession of 2007 to 2009 and represents the worst decline in jobs since the Great Depression in the 1930s.1 It is difficult to overstate how many jobs have been lost — each Labor Department report adds to the grim statistics.
In two short months, the leisure and hospitality industry, which includes travel, tourism, lodging and recreation, shed almost half its jobs.2 Most of the lost jobs were related to eating and drinking establishments, work that depends on disposable income and the ability of people to move around freely.3
Bureau of Labor Statistics data, cited by Charles Gascon, regional economist for the Federal Reserve Bank of St. Louis suggest that more than 66.7 million people working in food preparation, sales, production and services are now at high risk of layoffs.4
Conventional food production and delivery have been severely disrupted, but what about natural foods? I am a founding member of an exciting plan to keep organic farmers and natural product businesses up and running during this difficult time.
Are We Facing a Second Great Depression?
During the Great Recession, the greatest economic downturn in recent times, unemployment peaked at 10% in October 2009.5 During the Great Depression of the 1930s, that figure was 24.9%, which included people in work relief jobs.6 When you compare those figures with estimates of unemployment rates that may come from the COVID-19 pandemic that are between 10.5% and 40.6%, you see how serious this is.7
Many of us did not live through the Great Depression, but we have seen pictures of the devastating poverty and heard stories from our older relatives. People lacked both food and money, and bread lines and soup kitchens were how many survived. According to U.S. History.com, the food offerings began as charity operations:8
"When soup kitchens first appeared, they were run by churches or private charities. The Capuchin Services Center in southeast Detroit, for example, served 1,500 to 3,000 people a day. That center opened on November 2, 1929.
Volunteers of America also was important in setting up soup kitchens all over America. By the mid-1930s, state and federal governments also were operating them."
Today, charities are still feeding the growing number of hungry people. A few weeks into the COVID-19 pandemic, U.S. food banks were swamped. At an Omaha food pantry that before the pandemic normally served 100 people a day, 900 people a day show up now.9 In Las Vegas, the Three Square Food Bank, which anticipated 200 to 250 cars a day through the pandemic, is getting up to a 4-mile-long caravan of 500 to 600 cars, according to The New York Times.10
Today's pandemic food shortages also have parallels to World War II. During the war, the cost of munitions and war-related items caused the producer price index to rise by 17% and consumer price index by 10%, which raised the price of everyday staples.11 This led to passage of the Emergency Price Control Act of 1942, which authorized the U.S. government to ration food and set prices.12
In addition to stabilizing prices, the Emergency Price Control Act was meant to prevent hoarding and price gouging and ensure that scarce resources could reach everyone evenly.13 Among the rationed items that Americans could buy only with coupon books were sugar, coffee, processed foods, meats, fats, canned fish, cheese and canned milk.14
Flash forward to today's pandemic and food is again being rationed, as well as paper products and hand sanitizers.15 Store shelves are sometimes bare and people wait in long lines outside of grocery stores. During World War II, there were few fast food restaurants and people usually ate at home. During this pandemic, while many fast food restaurants are seeing long lines, home cooked meals are again becoming the norm, creating more demand for dry good items like pasta.
Big Food's Business Models Have Made Things Worse
Big Food's large dairies, packing plants and concentrated animal feeding operations (CAFOs) are struggling during the pandemic as consumer demand wanes and their nonregenerative business models abysmally fail. Milk is being dumped and edible livestock euthanized even as people are struggling with hunger and food insecurity.16 It is a thorough indictment of conventional agriculture.
According to Tim Gibbons, communications director at the Missouri Rural Crisis Center, COVID-19 is "shining a spotlight on the rigidity and lack of resilience for the corporate model of [farm production], which does not pay farmers fairly and is not good for consumers."17
It is ironic that despite the many systems' failures and even as Americans lose their livelihoods and face poverty, food insecurity and mental health crises, financial markets continue to rally. Ill-conceived government policies have clearly created a bubble that will crash in the future.
Conventional, nonregenerative farming is responsible for virtually every major environmental and health problem we now have, including:
|
Food insecurity and malnutrition amid mounting food waste |
Promotion of foodborne illnesses and drug-resistant bacterial infections |
|
Rising obesity and chronic disease rates despite growing health care outlays |
Rapidly dwindling fresh water supplies |
|
Toxic agricultural chemicals polluting air, soil and waterways, thereby threatening the entire food chain from top to bottom |
Disruption of normal climate and rainfall patterns due to the destruction of ecosystems by pollution |
Job Losses Worsen Poor Countries' Plights
In poor countries, COVID-19 presents even more dire consequences. People are not just at risk of illness and death with weak health care systems to treat them; they are also losing jobs because of the slowdown in Western countries' economies and less demand for the goods they manufacture and export.
A half-billion people who were not living this way before the pandemic may be catapulted into poverty, says Oxfam, a conglomerate of 19 organizations working to end global poverty.18 That is a 6% to 8% rise in poverty for the entire global population. According to Oxfam:19
"Existing inequalities dictate the economic impact of this crisis. The poorest workers in rich and poor nations are less likely to be in formal employment, enjoy labor protections such as sick pay, or be able to work from home.
Globally, just one out of every five unemployed people have access to unemployment benefits. Two billion people work in the informal sector with no access to sick pay — the majority in poor countries where 90 percent of jobs are informal compared to just 18 percent in rich nations."
In Bangladesh, more than 1 million garment workers, most of whom are women, have been laid off without pay because of cancellations of orders from Western clothing brands.20
In Africa, it is estimated that as many as half of all jobs could disappear. A taxi driver and father told Oxfam he had not had passengers since the lockdown closed the airport and restaurants, and added "This virus will starve us before it makes us sick."21
In India, as many as half a million people who had been working outside their cities of origin literally walked back home after their jobs disappeared with the COVID-19 pandemic.22 Amitabh Behar, chief executive of Oxfam India, called the exodus the "largest mass migration since independence."23
In Delhi, throngs of displaced workers coalesce at food lines set up by the government to feed them, but the amount of food is not always sufficient. "Instead of coronavirus, the hunger will kill us," said Nihal Singh, a migrant worker hoping to be fed at one of the food lines,24 echoing the sentiments of the African taxi driver who spoke to Oxfam. Clearly, famine is following on the footsteps of COVID-19.
The clustered food distribution in India and elsewhere also increases the risk of COVID-19 infections spreading, since the crowding and desperation of hungry people makes social distancing nearly impossible.
Introducing ‘The Nourish Mint’ — A New Way Forward
Even though natural products have rarely been in greater demand from consumers, COVID-19 has prevented natural products’ industry conferences that were normally scheduled from occurring. Such meetings, like the Natural Products Expo West, usually held the first week of March, facilitate connections and allow raw ingredient companies to pitch to brands, and brands, in turn, to pitch to independent retailers. Until now.
Luckily there is some good news when it comes to keeping the supply chain of natural foods and supplements flowing amid the temporary shutdown of such natural products’ industry conferences.
The Organic & Natural Health Association has created a new way for farmers and natural product businesses to interface called "The Nourish Mint."25 The online events, the first to take place June 18 and 25, 2020, at 4 p.m. to 5 p.m. Eastern time, will allow:26
"… brands, raw ingredient suppliers, distributors and independent retailers of SENPA, INFRA [Independent Natural Food Retailers Association], Positively Natural and MAHO [Mid-American Health Organization] to network and exchange new innovations and opportunities …
'Retailers are very interested in knowing not just about the product, but what goes into the product, where those ingredients come from and how they ultimately help the person buying it,' said Debra Short, executive director of SENPA. ‘The Nourish Mint’ is a great opportunity for them to do that while we wait for industry conferences to resume."
How does The Nourish Mint work? It will operate just like an in-person event in which raw ingredient companies and brands can present their products to an audience of independent retailers and other interested companies in the industry — except that it will be online. The presenters will have three minutes to showcase their products and three minutes to answer questions from the virtual audience.27
Flexibility is built into The Nourish Mint sessions. After the formal, live presentations of ingredients, products and brands, there will be an open social with attendees. Members of the audience will also be able to schedule individual or private meetings with the presenting companies for a future date.
The Nourish Mint format is unique because it involves the entire supply chain, says Karen Howard, the CEO and executive director of Organic & Natural Health Association.28
How to Participate in a Nourish Mint Event
Companies that are interested in presenting at a Nourish Mint event can apply by sending pitch materials to events@organicandnatural.org, on or before June 2, 2020. For members of Organic & Natural Health Association, the cost to present to prospective buyers is $300 and for non-members, it’s $500. Only 20 companies will be chosen to present at the June 18 and 25 sessions.29 Among the industry expert audience, who are called "mintors," will be:30
|
Heather Granato, VP of content, Informa |
Alan Lewis, VP government affairs, Natural Grocers |
|
Andrew Halpner, VP science and technical services, Atrium Innovations |
Greg Horn, co-founder of Nutritional Capital Network; director at William Hood and Co. |
|
Debra Short, executive director, SENPA |
Kantha Shelke, principle of Corvus Blue |
|
Anthony Zolezzi, chairman and co-founder UxHealth |
Corinne Shindelar, president emeritus, founder and former CEO INFRA |
Independent retailers who are members in good standing of SENPA, INFRA, Positively Natural and MAHO and Organic & Natural Health Association members may attend for free. Non-members may attend for $150 per session, and tickets can be acquired from the Organic & Natural Health Association.31
During the Pandemic Consider Growing Your Own Food
Growing your own vegetables and fruits is one of the best ways to ensure ready access to fresh, nutrient-dense and chemical-free food. It especially makes sense during this pandemic with its economic and food disruptions.
It is not true that you need a large space to grow a meaningful amount of food, though it is a popular misconception. In reality, "The Backyard Homestead" suggests you can grow enough organic food to feed a family of four on only a quarter-acre of land, all year round.32
In addition to supplying yourself with nutrient-dense, chemical-free food, a garden provides other important benefits. It gives you valuable and enjoyable physical exercise while exposing you to the UV rays so many people miss, especially during the COVID-19 shutdowns.
Gardening is also a natural antidepressant and anxiety reducer. According to a meta-analysis in Preventive Medicine Reports:33
"To our knowledge, this meta-analysis is the first to provide a quantitative synthesis of the evidence that gardening is beneficial for human health. Overall, the results suggest that participating in gardening activities has a significant positive impact on health.
Indeed, the positive association with gardening was observed for a wide range of health outcomes, such as reductions in depression and anxiety symptoms, stress, mood disturbance, and BMI, as well as increases in quality of life, sense of community, physical activity levels, and cognitive function."
The COVID-19 pandemic has created unemployment, poverty, food insecurity and a likely economic depression. The Nourish Mint is a ray of hope and a new way forward for farmers and natural product businesses during these troubling times.
from Articles https://ift.tt/3gFvfgd
via IFTTT
Quercetin Boosts Interferon Response to Viruses and COVID-19
As the number of people who have died from COVID-19 rises, more widespread testing reveals the infection may have moved farther and faster than was anticipated. The Centers for Disease Control and Prevention recently released five planning scenarios1 "designed to help inform decisions by modelers and public health officials who utilize mathematical modeling."
Each of the scenarios is based on numerical values and epidemiological characteristics of the viral infection, reflective of data gathered before April 29, 2020. The CDC is clear these are estimates and not predictions:2
- There was no known pre-existing immunity before 2019 so all people in the U.S. were assumed to be susceptible
- Between 20% and 50% of all people believed to be infected were asymptomatic; they were deemed likely to be infectious
- The "best estimate" is 0.4% of people who show symptoms will die; for people over 65 it's 1.3% and for those 49 and under it's 0.05%
Although there was nearly immediate pushback,3 estimates from The Centre for Evidence-Based Medicine at the University of Oxford were similar.4 There were two numbers used to define the percentage of deaths. The case fatality rate was chosen to represent the number of deaths divided by the number of confirmed cases; it was limited by the number of people tested.
Based on the possibility that up to 50% of those infected were asymptomatic, this created an abnormally high percentage. The infection fatality rate was used to represent the number of deaths divided by the number of people infected with SARS-CoV-2. That number was far lower since it included all people who are infected and not just those whose status was confirmed with a test.
The Centre acknowledges that estimating fatality rates in the early stages of infection is subject to uncertainty. However, it's important to note that the infection fatality rate in the 3,711 passengers on the Diamond Princess cruise ship — the ship quarantined in Yokohama for 27 days at the start of the pandemic5 — was 1.3%.6
Quercetin Boosts Cellular Response to Viruses
Even one death is too many. As I've written in the past, quercetin is a natural antihistamine and anti-inflammatory that lowers your risk for viral illnesses. In a recent paper, researchers identified one mechanism through which quercetin may work to control viral replication and promote health.7
Casein kinase II (CK2) is an enzyme with a diverse set of functions in the body. It is fundamental to controlling homeostasis at the cellular level. Yet, much of its functioning and mechanisms of action are still unknown.8 The enzyme is also involved in the survival and metastatic spread of cancer cells.
There is evidence that it down-regulates the ability a cell has to generate type 1 interferon when attacked by a virus. It does this by inhibiting retinoic acid-inducible gene I (RIG-I),9 which has protein sensors that signal genetic expression of type 1 interferon by identifying the replication of RNA viruses, such as SARS-CoV-2.
Researchers found that quercetin could inhibit the expression of CK2, which slowed the replication of RNA viruses in the lab and in mice.10 They pointed out that the effectiveness of supplemental quercetin may be hindered by the low solubility of the compound, which affects absorption.
By using "enzymatically modified isoquercitrin (EMIQ)" they discovered they could develop plasma levels 20 times higher than the same intake of unmodified quercetin. The authors concluded quercetin or EMIQ "should be included" in aiding the control of viral infections.
In research on the Ebola virus (EBOV) that triggered epidemics between 2013 and 2016, scientists found that the virus also suppressed type 1 interferon. They discovered that quercetin could suppress the effect on type 1 interferon and that it restored the body's ability to protect itself:11
"Overall, quercetin is the first identified inhibitor of the EBOV VP24 anti-IFN function, representing a molecule interacting with a viral binding site that is very promising for further drug development aiming to block EBOV infection at the early steps."
What Are Interferons?
Interferons (IFNs) are a subset of cytokines discovered in 1957.12 These cells are often the initial defense against viruses. There are two types and three forms of interferon. Within type 1 interferon, there are alpha and beta. Type II interferon has the gamma form.13
The different types are based on the function of the cytokine. Type I interferons help cells resist viruses. Type II aids in responding to infections and cancer growth. Initially, researchers hoped it could be used to treat diseases, including cancer. But it had serious side effects.
After further development, several forms were released to treat genital warts, multiple sclerosis and hepatitis B and C with varying results. The name "interferon" came from the ability of Type 1 to interfere with the virus's ability to duplicate. A cell secretes interferons when a foreign substance, like a virus, is detected.
However, the interferon does not function by attacking the virus. Instead, it tells the infected cell and the cells that surround the infected cell to make proteins that stop viral replication. Quercetin functions to stop CK2 from interfering with the action of type 1 interferon so cells are signaled to stop viral replication.
Quercetin Works With Zinc to Stem Viral Replication
Quercetin also functions as a zinc ionophore. This is a substance that helps transport zinc through the cellular plasma membrane14 and raises the level of zinc inside the cells. It's another mechanism through which quercetin may help lower the viral load and reduce the severity of viral infections.
Zinc has proven antiviral properties and can reduce the length of the average cold by 33%.15 Recently, scientists pointed out there were indications that maintaining normal zinc levels may help reduce the severity of COVID-19.16
In the lab, zinc has demonstrated the ability to inhibit replication of the SARS-CoV-2 virus, which researchers believe is the underlying therapeutic effect in the use of hydroxychloroquine.
Zinc may also up-regulate interferon production and the antiviral activity of the protein. Experts think it may reduce the risk of a secondary bacterial infection, especially against Streptococcus pneumoniae. Interestingly, zinc deficiency is common in older adults and in those who are obese, have diabetes or atherosclerosis.
Likely not by coincidence, these are some of the same populations who have a higher risk of severe disease from SARS-CoV-2.17 The research team who looked at past studies on zinc suggest that it has a protective effect against COVID-19 by lowering inflammation, helping clear mucus, preventing ventilator-induced damage and supporting immunity.18
In addition to the impact quercetin has on the immune system, researchers have also found it helps to ameliorate obesity, Type 2 diabetes, circulatory dysfunction, chronic inflammation and seasonal allergies.19 It has also been found to help lower blood pressure in patients with Stage 1 high blood pressure.20
Researchers have found that quercetin can trigger tumor regression and it can activate the mitochondrial pathway of apoptosis.21 This is programmed cell death, without which cells can grow uninterrupted and develop into cancerous growths.
Hydroxychloroquine: Poor Outcome With Added Risk
Two recent trials with the antimalarial drug hydroxychloroquine have yielded disappointing results. The first 75 patients at 16 Chinese treatment centers who were positive for COVID-19 were given hydroxychloroquine.22
The researchers found the primary endpoint of a reduction in the viral load, and secondary endpoints of improvement and reduction in clinical symptoms, were not significantly better than in the control group.
The group receiving hydroxychloroquine had a negative conversion of 85.4% compared to the control group of 81.3%. In addition, the group receiving hydroxychloroquine had a greater number of adverse events compared to the control group. The most common was diarrhea. The authors concluded:23
"The administration of HCQ did not result in a higher negative conversion rate but more alleviation of clinical symptoms than SOC [standard of care] alone in patients hospitalized with COVID-19 without receiving antiviral treatment, possibly through anti-inflammatory effects. Adverse events were significantly increased in HCQ recipients but no apparently increase of serious adverse events."
In a second study published in the Lancet,24 researchers used a multinational registry of patients who were given hydroxychloroquine or chloroquine, with or without a macrolide antibiotic for treatment. This class of antibiotic includes azithromycin, which has been used in other study groups.
There were 671 hospitals over six continents that supplied data of patients who were hospitalized between December 20, 2019, and April 14, 2020. During the study period there were 96,032 patients who met the criteria; 14,888 were in the treatment group and 81,144 were in the control group.
After controlling for confounding factors, the mortality rates were compared, and the researchers were unable to find a benefit from the antimalarial drugs when they were used alone or with a macrolide. What they did find was that using the:25
"… drug regimens was associated with decreased in-hospital survival and an increased frequency of ventricular arrhythmias when used for treatment of COVID-19."
A third observational study, published in The New England Journal of Medicine, found using hydroxychloroquine did not improve patient outcomes with COVID-19.26 In addition the FDA has cautioned against the use of hydroxychloroquine or chloroquine as an outpatient related to the dangerous heart arrhythmia side effects from the drugs.27
What is important to note in each of these studies is the absence of zinc in the intervention groups. We now know that chloroquine and hydroxychloroquine are zinc ionophores,28 which means the main ingredient required to prevent the viral infection may not have been given.
While it is difficult to make an assumption of the efficacy of treatment of COVID-19 with hydroxychloroquine, since zinc was not given in each of these studies, it is also important to consider the secondary side effects associated with the drug, namely ventricular arrhythmias.
Dose Recommendations for Zinc and Quercetin
During the COVID-19 pandemic and future infectious disease seasons, supplementing with quercetin and zinc may be a good idea for many. It can help boost your immune system's innate ability to ward off infectious illness. As for dosage, here are some basic recommendations:
• Quercetin — According to research from Appalachian State University in North Carolina, taking 500 mg to 1,000 mg of quercetin per day for 12 weeks results in "large but highly variable increases in plasma quercetin … unrelated to demographic or lifestyle factors."29
• Zinc (and copper) — When it comes to zinc, remember more is not better. In fact, it can backfire. When taking zinc, you also need to be mindful of maintaining a healthy zinc-to-copper ratio. Chris Masterjohn has a Ph.D. in nutritional sciences.30 He's written about the relationship between zinc and copper, saying:31
"In one study, 300mg/day of zinc as two divided doses of 150 mg zinc sulfate decreased important markers of immune function, such as the ability of immune cells known as polymorphonuclear leukocytes to migrate toward and consume bacteria.
The most concerning effect in the context of COVID-19 is that it lowered the lymphocyte stimulation index 3-fold. This is a measure of the ability of T cells to increase their numbers in response to a perceived threat.
The reason this is so concerning in the context of COVID-19 is that poor outcomes are associated with low lymphocytes … the negative effect on lymphocyte proliferation found with 300 mg/day and the apparent safety in this regard of 150 mg/d suggests that the potential for hurting the immune system may begin somewhere between 150-300 mg/d.
It is quite possible that the harmful effect of 300 mg/d zinc on the lymphocyte stimulation index is mediated mostly or completely by induction of copper deficiency.
The negative effect of zinc on copper status has been shown with as little as 60 mg/d zinc. This intake lowers the activity of superoxide dismutase, an enzyme important to antioxidant defense and immune function that depends both on zinc and copper.
Notably, the maximum amount of zinc one could consume while staying in the acceptable range of zinc-to-copper ratios and also staying within the upper limit for copper is 150 mg/d."
from Articles https://ift.tt/2Mna0Sp
via IFTTT
7 of the best fat-burning lunches to meal prep this week
From burrito bowls to high-protein pumpkin soup, here are seven healthy lunches that will help you put your body into fat-burning mode, all approved by dietitian Melissa Meier.
from Nutrition | body+soul https://ift.tt/3clU2CO
from Nutrition | body+soul https://ift.tt/3clU2CO
Sorry but going keto might make you gain weight, in the long run
Dietitian Susie Burrell spoke with Professor Grant Brinkworth, a senior research scientist from CSIRO, about the negative side effects of the Keto diet on weight loss. And apparently, the popular diet could lead to long term weight gain - not loss.
from Diet | body+soul https://ift.tt/2ZTOKf7
from Diet | body+soul https://ift.tt/2ZTOKf7
6 best sexy workouts to tone from home
Get toned, feel sexy and boost your confidence with these saucy — and effective — online workouts.
from Fitness | body+soul https://ift.tt/2XiHzLK
from Fitness | body+soul https://ift.tt/2XiHzLK
Is it OK to sleep in undies?
Our resident doctor answers the age old question - do you really need to let it ‘breathe’ down there?
from Health | body+soul https://ift.tt/2zQwIzL
from Health | body+soul https://ift.tt/2zQwIzL
The appliance that makes healthy meal prepping a breeze
Love meal prepping, but wish it were easier? A slow cooker is the kitchen appliance you need.
from Nutrition | body+soul https://ift.tt/2XLEEKO
from Nutrition | body+soul https://ift.tt/2XLEEKO
5 winning ways for kids burn energy
Could your kids power the electrical grid, if you could only figure out how to tap that energy? Someday, all the hours spent cooped up at home will be a memory, not a daily reality. But if your children are bouncing off the walls with schools and day care still closed and summer coming, here are five active ideas to safely channel their energy. Pandemic or not, preschoolers benefit from active play throughout the day, and children ages 6 to 17 should rack up at least 60 minutes of activity daily, according to the Centers for Disease Control and Prevention. And since regular activity boosts health and lifts mood, everyone stands to benefit.
Pick a card
Annelieke Rietsema, an employee health coach and fitness specialist at Newton-Wellesley Hospital, suggests this simple strategy. Take a pack of playing cards and assign different exercises to each suit. For example, hearts could be jumping jacks or bear crawl; diamonds could be burpees or somersaults (if you have room); spades could be mountain climbers or cat-cow; clubs could be knee pushups or squats. Now shuffle or mix up the cards (face down), then start going through the deck. Kids do the number of each exercise on cards numbered 2 to 9. They do 10 of an exercise if a card is an ace, jack, queen, or king. So, a jack of hearts in the spades suit could equal 10 mountain climbers. For an exercise without discrete repetitive movements, like the bear crawl, try assigning a number of seconds based on the card selected (a five of hearts equals five seconds of bear crawl).
Children can do the shuffling and assign exercise choices, even picking simpler or harder exercises depending on age or ability.
Top of the hour
Five-minute or 10-minute energy burns at the top of each hour may help keep the peace. Have kids set a timer and choose easy exercises: running in place, jumping jacks, skipping rope, practicing sit-ups and squats. Children can compete with each other or with friends — from one week to the next, is it getting easier to do certain exercises? Can you do more than you could before?
Creature moves
Challenge younger children to think up and enact the moves of animals and other creatures: waddle like a duck, small hops like a bunny, giant hops like a kangaroo, slither like a snake, jump high like a frog, crawl-walk like a bear, inch forward like a turtle, waggle-dance like a honeybee, flap arms like a bird, crawl sideways like a crab, and so on. Set up indoor races for the quieter moves (crab, duck, snake) and occasional outdoor races for louder critters, to see who reaches the finish line in the least and most time. Extra points for unusual choices.
Personal best
Record how long a child can hop or balance on one foot or the number of push-ups, sit-ups, jumping jacks, or other exercises a child can do in a row. Practice three times a week and track the results once weekly.
Teens and some younger children may enjoy setting goals and logging progress in virtual races. The Healthy Kids Virtual Running Series for children in pre-K to grade 8 has a state-by-state locator to find local races. Many charities are encouraging people of all ages to raise money while walking, running, biking — or even dancing — in virtual events.
Yoga and fitness classes online
Two engaging options are Cosmic Kids, which combines yoga and storytelling into a calming, enjoyable workout for many children, and Go Noodle, which has high-energy video or app games to get kids moving and silly costumes to amuse them. Or you can find free online options, or sample classes available through local gyms, recreation centers, or YMCAs. Be sure to screen fitness videos aimed at children, to check if they are appropriate for your child.
Whatever you choose to help children burn energy, do give a thought to your neighbors. Quieter exercises are best if you live above someone, and mixing in safe outdoor time is good for everyone, parents included. If there’s enough room to move freely while maintaining safe distances, a game of tag or soccer, a bike ride, or just a run, skip, or kangaroo-hop to the end of each block could be fun.
The post 5 winning ways for kids burn energy appeared first on Harvard Health Blog.
from Harvard Health Blog https://ift.tt/2XjUzB6
Vitamin D Combats Viral Infections and Boosts Immune System
In this interview, I interview three vitamin D experts about the importance of vitamin D for improving your immune function and resistance to viral infections of all kinds, including COVID-19.
Bruce Hollis, Ph.D., with the Medical University of South Carolina, has researched vitamin D since the late 1970s. His research associate at the Medical University of South Carolina is Dr. Carol Wagner, who is a neonatologist and has been researching vitamin D since 2000.
Carole Baggerly is the director and founder of GrassrootsHealth Nutrient Research Institute, a nonprofit public health research organization dedicated to moving public health messages regarding vitamin D from research into practice. Baggerly received our Game Changer Award in 2018. She started her work in vitamin D after treatment for breast cancer in 2005.
Vitamin D Levels Correlate With Disease Severity
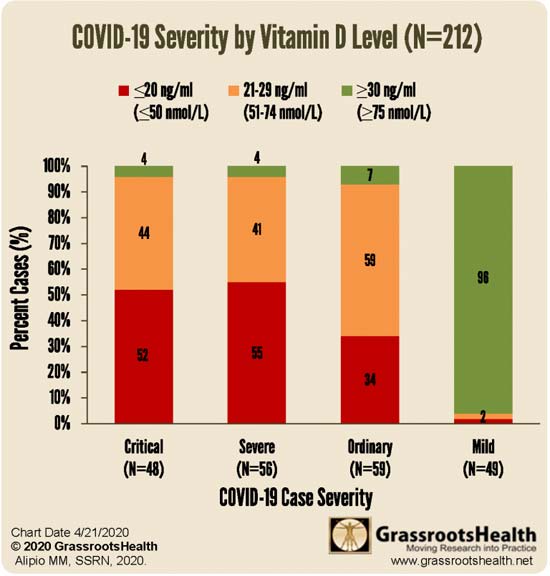
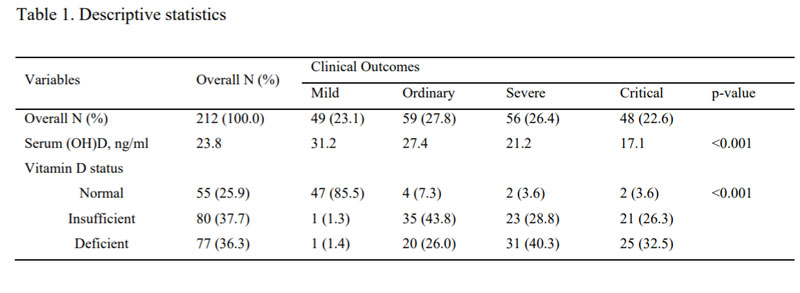
GrassrootsHealth recently conducted a review of an observational study involving 212 patients in Southeast Asia who had COVID-19, identifying a correlation between vitamin D levels and disease severity. Those with the mildest disease had the highest vitamin D levels, and vice versa.
Of the 212 people, 49 had mild disease; 59 had ordinary disease; 56 were severe and 48 were critical. In the initial study group of 212 patients (see Table 1 below), 55 had normal vitamin D levels, which was defined as greater than 30 ng/ml; 80 had insufficient levels of 21 to 29 ng/ml and 77 had deficient levels of less than 20 ng/ml.
Now, it’s worth noting that the “optimal” vitamin D level in that study was set at 30 nanograms per milliliter (30 ng/mL), which may actually be suboptimal. According to the research done by GrassrootsHealth, 40 ng/mL is the lower edge of optimal, with 60 ng/mL to 80 ng/mL being ideal for health and disease prevention. Despite that, the benefit of having a vitamin D level above 30 ng/mL was clear.
Vitamin D Levels Correlate With Mortality Risk
A second study looked at the data from 780 hospital patients in Indonesia. The same vitamin D level cutoffs were used in this study: below 20 ng/mL; between 20 ng/mL and 30 ng/mL; and above 30 ng/mL.
After adjusting for confounding factors, those with a vitamin D level between 20 ng/mL and 30 ng/mL had a sevenfold higher risk of death than those with a level above 30 ng/mL. Having a level below 20 ng/mL was associated with a 12 times higher risk of death. As noted by Hollis, “That's really strong data.”
It’s Your Vitamin D Blood Level That Matters, Not the Dose
Now, many vitamin D studies conclude that vitamin D supplementation has little or no effect on any given health problem or condition. But there’s a very simple reason for this: Virtually every one of these studies use the same dosage or dosages for everyone, and do not measure participants’ blood levels.
This is a crucial mistake, as it’s really the blood level that needs to get over a particular threshold, and the dosage required to get there can vary widely. Another problem is the fact that most studies use far too low a dosage. If the dosage is too low, you cannot get your blood level into the protective range, and thus it will appear as though vitamin D is useless.
A third factor that can influence the outcome of vitamin D studies is the interaction between vitamin D and other nutrients. Competing deficiencies can affect a particular sub cohort or population, thereby obfuscating results.
A fourth factor is how you define deficiency — using a “word” versus a serum level. For the GrassrootsHealth Scientists’ Panel of 48 researchers, the consensus is that minimum serum level should be 40 ng/ml (100 nmol/L). Wagner explains:
“If you do a PubMed search, you see literally thousands of articles. You see this really rich basic science information that's been accumulating in the last two decades, that strongly supports vitamin D's role in immunity.
But then, when randomized control trials are done, there are some that suggest vitamin D is effective and others say no. It's been a contentious issue and I'm sure Bruce and Carole [Baggerly] will agree with me that doing nutrients studies is not the same as doing a pharma study where … they start with zero as their baseline.
[When it comes to] vitamin D [levels], everybody is different. And so, using a biomarker, which is what we use in our studies, total circulating 25(OH)D is a much better indicator.”
Hollis adds:
“In nutrient studies with vitamin D, it's always been the dosage — how much you're going to give — with no concern about what the attained blood levels would be.
In our studies, of course, we always measure blood levels. Those studies that Carol [Wagner] and I carried out in pregnancy (in 2003), they were monitored by the FDA. We had to get an investigational drug number (IDN) to run these studies, and it was unheard of to have to do that …
In the end, we proved the [dosage] we [gave] — 4,000 units — was totally harmless as far as dosing went. But it's still a fight … We have yet to see one adverse event due to vitamin D in any of the studies that Carol [Wagner] and I have carried out, not a single one …”
Laws Need Updating
Unfortunately, with labeling laws the way they are, it’s very difficult to get this point across. As noted by Baggerly:
“GrassrootsHealth … [asked] the FDA … for the ability to be able to print on the [label of] any vitamin D supplement that ‘[Vitamin D] may help have a healthy pregnancy and [improve] birth outcomes.’ What we were told in that meeting by the FDA person was, ‘According to what dose?’
We explained repeatedly that it wasn't a dose, it was a serum level, and the FDA person in charge said, ‘By law, we can only accept recommendations based on dose, and if you can't provide us with a dose, we cannot accept any recommendation.’ So, the laws are out of date, to say the least.”
Skin Color Impacts Your Vitamin D Deficiency Risk
The color of your skin has correlations to your vitamin D level, and we’re also seeing racial disparities in COVID-19. As noted by Hollis, in Detroit, Michigan, where African-Americans account for 14% of the population, they accounted for 40% of COVID-19 deaths.1
“It was even worse in Sweden where the Somali population is less than 1%, and they [account for] 40% of the deaths,” Hollis says. “In Britain, of the 24 health care physicians who have died, 23 were people of color. It was so bad that they pulled those people off the front lines … the physicians and the nurses.”
Vitamin D deficiency likely plays a role in this racial disparity, although nutrition, obesity and diabetes rates also contribute to immune dysfunction. It’s important for people with darker skin to realize that the more melanin you have, the more sun exposure you require to make sufficient amounts of vitamin D.
According to Hollis, it’s physiologically impossible for a dark-skinned individual in the United States, unless they're in Southern Florida or Hawaii, to get optimal vitamin D from typical sun exposure.
Daily Supplementation May Strengthen Lung Tissue
If for whatever reason you cannot get regular sun exposure, then vitamin D supplementation is advisable. Ideally, you’ll want to take it daily, opposed to taking a large bolus dose once a week or once a month. As noted by Hollis, studies have consistently shown only daily supplementation were effective.
“When they looked at bolus supplementation, the effect on respiratory infection disappeared,” he says. “Taking a bolus dose every other week or once a month, every three months, that was not effective at controlling respiratory infections. So, we prefer daily [supplementation].”
Baggerly adds:
“The vitamin D component produced in the skin as a result of sun exposure is at one stage what we take as a supplement, the D3, and that then is metabolized into 25(OH)D, which is what we're measuring, for the most part.
The D3 and even the 25(OH)D have been considered in times past … as not being active … In recent studies, and we really are talking relatively recent, the D3 itself seems to be active in helping keep the epithelia strong [to prevent endothelial leakage].”
Vitamin D3’s ability to strengthen the endothelial structure of the lungs may be one way in which vitamin D helps protect against COVID-19. “COVID-19 attacks the lungs … and vitamin D in this model showed to stabilize that,” Hollis says.
Vitamin D Strengthens and Regulates Immune Function
Vitamin D also has a clear effect on your innate immune system, which is your first line of defense against bacteria and viruses, as well as your adaptive immune system, which involves your T regulatory helper and suppressor cells, and natural killer cells.
All of these need to be in balance, Wagner explains. If an imbalance occurs, you can end up with a cytokine storm. According to Wagner, vitamin D is very effective for regulating and balancing adaptive immunity. One example demonstrating the elegance of this system is pregnancy. Wagner explains:
“You go from a very active immune system where you have, as the egg is fertilized, an invasion into the uterine wall. You have to allow for that, [and] it's a very pro-inflammatory state. Then, in order to allow fetal growth, you have to have quiescence of that [proinflammatory state].
You see shifts in the T cell populations, the phenotypes, as well as in the monocyte macrophage population, their activity. And then, at the time of delivery, you shift back to a proinflammatory state [when you] go into labor and have expulsion of the fetus and the placenta. So, it's a tremendously elegant process.
We know that when it's deranged, we get such conditions as preeclampsia. You get a vasculitis throughout the body and it can lead to death of both the mother and the fetus, and you have a cytokine storm during that. So COVID-19 is not like a foreign alien; it's utilizing the very immune system that we have in our body and it makes sense.
Even though this particular virus is new, it's incorporating systems within our body that are ancient and that includes a very ancient pre-pro hormone, which is vitamin D.
So, it makes sense to me, as a physician and as a scientist, that those individuals who have balance in their bodies, and in this case vitamin D balance, they're going to do better than if they had deficiency [because then] they can't mobilize those [immune] cells. Those cells are going to be dysfunctional.”
Research has also demonstrated that pregnant women with optimal vitamin D levels significantly reduce their child’s risk of developing Type 1 diabetes, which is an autoimmune disorder. As noted by Baggerly:
“We're working with the Diabetes Research Center to see whether, even after the child is born, as long as they don't have full-blown type 1 diabetes, what can we do to help stop it? And it turns out that the combination of vitamin D and omega-3 really matters.”
The Importance of Vitamin D Testing
Naturally, vitamin D has many other benefits beside boosting immune function and protecting against respiratory diseases and viral infections. Wagner, for example, reviews some of the benefits in pregnancy and delivery, so for more information, be sure to listen to the interview.
As mentioned, the most important factor here is the level of vitamin D in your blood, not the daily dose, so it’s important to get tested at least twice a year. Again, you want a level of at least 40 ng/mL, and ideally between 60 ng/mL and 80 ng/mL.
According to data published in the Archives of Internal Medicine,2 75% of American adults and teens are deficient in vitamin D, based on a sufficiency level of 30 ng/mL. If the sufficiency cutoff were to be moved to 40 ng/mL or 60 ng/mL, deficiency rates in the U.S. would likely be in the high 90% bracket.
Importantly, aside from people with darker skin, the elderly tend to lose the ability to synthesize vitamin D from sun exposure, and therefore tend to have suboptimal levels even if they spend plenty of time outdoors. “It's at that point people may need to supplement or find additional sources,” Baggerly says.
One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in the GrassrootsHealth’s personalized nutrition project, which includes a vitamin D testing kit, either alone or in combination with the omega-3 test. This is done in the convenience of your home.
You’ll learn your nutrient levels, how effective your health actions are, and you’ll be able to see 1000’s of other data sets that allow you to compare health outcomes important to you.
The Synergy Between Magnesium and Vitamin D
If your vitamin D level is low and remains low even though you’re taking high dosages every day, say around 5,000 to 10,000 IUs, you may be too deficient in magnesium for your body to convert the vitamin D into its active form. As explained by Hollis:
“A couple of years ago, I was reviewing an epidemiologic study from Harvard that showed the relationship between magnesium intake [and vitamin D levels]. Because you can't do a blood test to tell if you have enough magnesium … you have to take it every day. At the time … I was taking 10,000 IUs of vitamin D a day and I couldn't get my blood levels to go up to 50 ng/mL.
And so I thought, wow, so I'm going to start taking magnesium. So, I start taking 400 mg a day and my level is now 60 ng/mL on 6,000 IUs of vitamin D a day. So, magnesium intake can have profound effects on the conversion into 25D … The magnesium intake is really important and I never paid much attention to that until then.”
GrassrootsHealth now also has a magnesium research project called Magnesium* PLUS Focus, which is also open for enrollment. All of these nutrient field trial projects involve sending in a blood spot test that you do at home, and filling out a health questionnaire and providing details on the supplements you take.
COVID-19 Study Underway
Last but not least, GrassrootsHealth is currently working on a vitamin D study to assess its ability to prevent COVID-19 and/or reduce illness severity. Wagner explains:
“We put together a study that will be submitted to our human subjects committee shortly. And we're working with GrassrootHealth on this. We're taking individuals who come to our virtual clinics for COVID-19 testing. Those who are negative at the time of testing … [will] get randomized to receive 6,000 IUs a day of vitamin D or placebo.
Everyone will take 800 IUs a day of vitamin D in the form of a multivitamin that also has magnesium, vitamin C and the B vitamins. Then, we follow them monthly for retesting and if they become positive, we'll note that and the severity of their symptoms and their duration of the acute illness. Every month, we’ll test their vitamin D [25(OH)D] level, and along with that we're measuring their COVID-19 PCR … [and] antibodies …
In the COVID positive arm … they would get a bolus of 20,000 IUs a day for three days followed by 6000 IU/day vs. placebo. All would take the multivitamin, which has 800 IUs plus the other vitamins …
The endpoints [are]: severity of symptoms and whether they required hospitalization, how long was it before they could return to their normal daily activities … respiratory questionnaires and … nasal drainage. They're actually doing genotyping of the cells in the secretions from the nose and so forth in those individuals.
A key measure though, of the vitamin D, is the desired [level] of at least 40 ng/mL. So those who have not achieved that in two months' time, their doses are going to be adjusted to get there. It's [the focus is] not going to be the dose.”
REALLY IMPORTANT: Optimize Your Vitamin D Levels Before Fall!
Not only will be this an important strategy for you and your family, but it would be really helpful to start thinking about your community. People of color are at really high risk because their skin color impairs their ability to generate vitamin D from sun exposure. So if you could speak to any pastors in churches with large congregations of people of color and help them start a program getting people on vitamin D you could help save many lives, far more than any vaccine program.
Additionally, if you have a family member or know anyone who is in an assisted living facility you could meet with the director of the program and encourage them to get everyone tested or at least start them on vitamin D. Tomorrow I will have an article with more specific action steps, so you can start planning now.
For years, I’ve stressed the importance of optimizing your vitamin D level, especially in anticipation of flu season, and it seems clear it can go a long way toward protecting yourself against COVID-19 as well. Wagner notes:
“One of the things that I think is worth mentioning is there are receptors all over the body for vitamin D and it includes the Type II cells [in the lungs], which create surfactant.
So, the issue of whether or not an infection gets from upper respiratory down into the lung. That's when it progresses from upper respiratory to lower respiratory, and it's the lower respiratory infection that's associated with cytokine storm …
Vitamin D has a tremendous effect on the local renin-angiotensin system. You've probably heard about ACE2 [receptors] and so forth. Vitamin D specifically affects surfactant production — this local renin-angiotensin system that is involved with fluid clearance … When you have vitamin D deficiency, that whole system is deranged.”
In closing, experts are already warning that SARS-CoV-2 may reemerge in the fall when temperatures and humidity levels drop, thereby increasing the virus’ transmissibility. Now is the time to check your vitamin D level and start taking action to raise it if you’re below 60 ng/mL.
Again, an easy and cost-effective way of measuring your vitamin D level is to order GrassrootsHealth’s vitamin D testing kit and learn more about vitamin D and its impact on your health. Knowledge is empowerment, and that is particularly true during this pandemic.
from Articles https://ift.tt/3djGhWB
via IFTTT
Benefits of social networks to disaster response questioned
Faced with a common peril, people delay making decisions that might save lives, fail to alert each other to danger and spread misinformation. Those may sound like behaviors associated with the current pandemic, but they actually surfaced in experiments on how social networks function in emergencies.
from Top Health News -- ScienceDaily https://ift.tt/3duJFha
from Top Health News -- ScienceDaily https://ift.tt/3duJFha
COVID-19 patients who undergo surgery are at increased risk of postoperative death
Patients undergoing surgery after contracting coronavirus are at greatly increased risk of postoperative death, a new global study reveals. Researchers found that amongst SARS-CoV-2 infected patients who underwent surgery, mortality rates approach those of the sickest patients admitted to intensive care after contracting the virus in the community.
from Top Health News -- ScienceDaily https://ift.tt/2zKZdiq
from Top Health News -- ScienceDaily https://ift.tt/2zKZdiq
How the coronavirus could be prevented from invading a host cell
How might the novel coronavirus be prevented from entering a host cell in an effort to thwart infection? A team of biomedical scientists has made a discovery that points to a solution. The scientists report that two proteases -- enzymes that break down proteins -- located on the surface of host cells and responsible for processing viral entry could be inhibited.
from Top Health News -- ScienceDaily https://ift.tt/2MfmlYU
from Top Health News -- ScienceDaily https://ift.tt/2MfmlYU
Scientists develop method to help epidemiologists map spread of COVID-19
Scientists have developed a method they believe will help epidemiologists more efficiently predict the spread of the COVID-19 pandemic. Their new study outlines a solution to the SIR epidemic model, which is commonly used to predict how many people are susceptible to, infected by, and recovered from viral epidemics.
from Top Health News -- ScienceDaily https://ift.tt/2MdZw83
from Top Health News -- ScienceDaily https://ift.tt/2MdZw83
B+S LIVE: Soothing Sunday mediation with Elise Catchlove
Close down your eyes and let Elise Catchlove take you through a calming Sunday mediation.
from Fitness | body+soul https://ift.tt/3gxjUit
from Fitness | body+soul https://ift.tt/3gxjUit
The fight goes on: Clinical trial shows promising new treatment for rare blood cancer
Although lymphoma is one of the most common types of blood cancer, it has a rare subtype for which no effective treatment regimens are known. For the first time, researchers have conducted clinical trials for a new treatment protocol and report it to be quite promising.
from Top Health News -- ScienceDaily https://ift.tt/36Lr12n
from Top Health News -- ScienceDaily https://ift.tt/36Lr12n
Key player in hepatitis A virus infection
Researchers designed experiments using gene-editing tools to discover how molecules called gangliosides serve as de facto gatekeepers to allow the virus entry into liver cells and trigger disease.
from Top Health News -- ScienceDaily https://ift.tt/2MfEg1y
from Top Health News -- ScienceDaily https://ift.tt/2MfEg1y
Adolescent exposure to anesthetics may cause alcohol use disorder, new research shows
Early exposure to anesthetics may make adolescents more susceptible to developing alcohol use disorder (AUD), according to new research.
from Top Health News -- ScienceDaily https://ift.tt/2zBuHrl
from Top Health News -- ScienceDaily https://ift.tt/2zBuHrl
'Single pixel' vision in fish helps scientists understand how humans can spot tiny details
Recently discovered 'single-pixel vision' in fish could help researchers understand how humans are able to spot tiny details in their environment -- like stars in the sky.
from Top Health News -- ScienceDaily https://ift.tt/2TUAmPX
from Top Health News -- ScienceDaily https://ift.tt/2TUAmPX
Study charts developmental map of inner ear sound sensor in mice
A team of researchers has generated a developmental map of a key sound-sensing structure in the mouse inner ear. Scientists analyzed data from 30,000 cells from mouse cochlea, the snail-shaped structure of the inner ear. The results provide insights into the genetic programs that drive the formation of cells important for detecting sounds and the underlying causes for some forms of inner ear hearing loss.
from Top Health News -- ScienceDaily https://ift.tt/2TOgrCn
from Top Health News -- ScienceDaily https://ift.tt/2TOgrCn
Why Was Wuhan Lab Locked Down When Outbreak Began?
As reported in "Bioweapon Labs Must Be Shut Down and Scientists Prosecuted," there's mounting evidence suggesting SARS-CoV-2 may have been leaked (whether inadvertently or not) from the biosafety level (BSL) 4 laboratory in Wuhan, China.
Secretary of State (and former CIA chief) Mike Pompeo has gone on record stating "the coronavirus originated in a lab in Wuhan," and has accused China of covering up the leak.1,2
I've also interviewed bioweapons expert Francis Boyle and molecular biologist Judy Mikovits, both of whom have cited evidence that strongly points toward SARS-CoV-2 being an escaped laboratory creation.
Why Was Wuhan Lab Shut Down?
Fueling suspicions that SARS-CoV-2 escaped from the lab in Wuhan — and that it began far earlier than admitted — is an analysis3 of commercial telemetry (i.e., cellphone) data showing a significant and unusual reduction in device activity in and around the Wuhan Institute of Virology's (WIV) National Biosafety Laboratory during October 2019.4,5,6
According to the open source telemetry report,7 "Beginning on October 11, there was a substantial decrease in activity," and "the last time a device is active prior to October 11 is October 6."
Between October 14 and October 19, there was no device activity in the area around the laboratory at all. "During this time, it is believed that roadblocks were put in place to prevent traffic from coming near the facility," the report states. What's more, between October 7 and October 24, there was no activity within the facility itself.
While not concrete proof of a biohazard leak, the absence of cellphone traffic in and around the laboratory in October 2019 suggests the lab may have been shut down for a period, and the roads around it blocked off. The question is why?
Amid accusations that the World Health Organization helped suppress information about the pandemic on behalf of China, a review of its handling of the COVID-19 pandemic will be conducted,8 although it is still unclear which body will conduct the review and when. Many are also asking just how independent such a review will or can be.
What Kinds of Experiments Were Done at Wuhan Lab?
A crucial piece of the lab release hypothesis that is missing from media reports and scientific opinion is a clear description of the experiments being conducted at the WIV. WIV researchers have engineered chimeric viruses where the gene for the cell entry protein (S protein receptor-binding domain) from one virus is replaced by that of another virus.
In a May 16, 2020, article,9 Fabio Carisio, founder and editor-in-chief of the Italian Christian news site, GospaNews, reviewed, in chronological order, experiments involving chimeric superviruses conducted at WIV and the governments that funded them.
As described in one 2017 study published in PLOS Pathogens,10 "Cell entry studies demonstrated that three newly identified SARSr-CoVs with different S protein sequences are all able to use human ACE2 as the receptor, further exhibiting the close relationship between strains in this cave and SARS-CoV."
The goal of these experiments has been to identify what determines a virus' ability to enter into a human cell. The extension of these experiments is to infect living animals with these chimeric viruses to evaluate the factors that determine disease symptoms and spread.
One of the authors of that 2017 PLOS Pathogens study was Dr. Shi Zheng-Li, director of WIV, also known as the "bat woman," as she's been China's leading researcher of bat coronaviruses.11 Zheng-Li and WIV have had a long-standing collaboration with Peter Daszak, Ph.D., and the EcoHealth Alliance Inc. in New York City, which Daszak is also the president of.12
EcoHealth Alliance is a U.S. pandemic prevention group. Daszak is also chairman of the Forum on Microbial Threats at the National Academies of Sciences, Engineering and Medicine,13 a private nonprofit that advises government on scientific matters and is funded by Congress, federal agencies and philanthropic organizations.14
Daszak is currently leading a project to continue these potentially dangerous animal experiments,15 and it's worth noting that he has also been one of the most prominent and vocal critics of the lab release hypothesis.
On a side note, 60 Minutes recently reported16 the White House Administration cut Daszak's funding in late April 2020 — funding that, according to Daszak, had been instrumental during Gilead's development of the antiviral drug Remdesivir,17 which is now being promoted as a treatment for COVID-19.
Remdesivir's development was sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), which is led by Dr. Anthony Fauci. Fauci is also a board member18 of the Global Preparedness Monitoring Board (GPMB).
GPMB is an organization that claims to be an independent monitoring and accountability body but is in fact part and parcel of the World Health Organization and The World Bank, and receives funding from the Bill & Melinda Gates Foundation.19 You can learn more about these sordid connections, and why they matter, in "Global Health Mafia Protection Racket."
Another Paper Questions Natural Evolution Theory
As mentioned, a number of experts have weighed in on the science of SARS-CoV-2's origin by analyzing its genetic code. Perhaps two of the clearest expositions on this have been published by Chris Martenson,20 Ph.D., and Yuri Deigin.21 Another paper prepublished May 2, 2020, ahead of peer-review, points out:22
"In a side-by-side comparison of evolutionary dynamics between the 2019/2020 SARS-CoV-2 and the 2003 SARS-CoV, we were surprised to find that SARS-CoV-2 resembles SARS-CoV in the late phase of the 2003 epidemic after SARS-CoV had developed several advantageous adaptations for human transmission.
Our observations suggest that by the time SARS-CoV-2 was first detected in late 2019, it was already pre-adapted to human transmission to an extent similar to late epidemic SARS-CoV. However, no precursors or branches of evolution stemming from a less human-adapted SARS-CoV-2-like virus have been detected.
The sudden appearance of a highly infectious SARS-CoV-2 presents a major cause for concern that should motivate stronger international efforts to identify the source and prevent near future re- emergence. Any existing pools of SARS-CoV-2 progenitors would be particularly dangerous if similarly well adapted for human transmission …
Even the possibility that a non-genetically-engineered precursor could have adapted to humans while being studied in a laboratory should be considered, regardless of how likely or unlikely."
Anonymous Scientist Accuses Zheng-Li of Scientific Fraud
Getting back to Zheng-Li, she increasingly appears to be a key figure in the discussion as to whether SARS-CoV-2 is of natural origin or not. January 23, 2020, she published a paper23 in the journal Nature, titled "A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin," in which she compared the genetic sequence of SARS-CoV-2 to other coronaviruses and delineated its evolutionary path.
According to Zheng-Li and her co-authors, SARS-CoV-2 "is 96% identical at the whole-genome level to a bat coronavirus" called RaTG13. They further claim they could find "no evidence for recombination events was detected in the genome of 2019-nCoV."24 The disturbing thing about this bat coronavirus, RaTG13, is that it appears to have the ability to infect humans.
These findings are now being rebuked by an anonymous — possibly Chinese — researcher who has published25 an alternative theory in a blog called Nerd Has Power and refers to him or herself as "A nobody scientist."26
The blog post in question has been discussed by GM Watch,27 Australian science writer Joanne Nova28 and Steven Mosher,29 president of the Population Research Institute (a nonprofit research group that exposes human rights abuses and the myth of overpopulation30), who noted that:
"Because he published his raw data, I and others have been able to check and verify his work." Mosher goes on to present "a summary of one of the blogger's critiques, in the hope of making the blogger's general line of argument accessible to the layman."
The unnamed blogger writes, in part:31
"As stated in the paper, RaTG13 was discovered from Yunnan province, China, in 2013. According to credible sources, Shi has admitted to several individuals in the field that she does not have a physical copy of this RaTG13 virus.
Her lab allegedly collected some bat feces in 2013 and analyzed these samples for possible presence of coronaviruses based on genetic evidence. To put it into plainer words, she has no physical proof for the existence of this RaTG13 virus. She only has its sequence information, which is nothing but a string of letters alternating between A, T, G, and C.
Can the sequence of such a virus be fabricated? It cannot be any easier. It takes a person less than a day to TYPE such a sequence (less than 30,000 letters) in a word file. And it would be a thousand times easier if you already have a template that is about 96% identical to the one you are trying to create.
Once the typing is finished, one can upload the sequence onto the public database. Contrary to general conception, such database does not really have a way to validate the authenticity or correctness of the uploaded sequence.
It relies completely upon the scientists themselves — upon their honesty and consciences. Once uploaded and released, such sequence data becomes public and can be used legitimately in scientific analysis and publications."
Was Evidence for Natural Evolution Fabricated?
In other words, this anonymous individual claims Zheng-Li fabricated the genetic code of the RaTG13 virus, and that it doesn't actually exist. The blogger points out that had Zheng-Li in fact discovered a bat coronavirus in 2013 capable of infecting humans, it would have been a groundbreaking discovery.
Alas, she never published such a paper. Instead, she "made her fame in the coronavirus field by publishing in Nature32 two bat coronaviruses (Rs3367 and SHC014)," the unnamed blogger writes.33 That paper, published in 2013, showed SARS was likely of bat origin, and that it uses the ACE2 receptor for cell entry.
"… she only needed to take one peek at the sequence of RaTG13's RBD [RNA binding domain] and immediately realize: this virus closely resembles SARS in its RBD and has a clear potential of infecting humans.
If Shi's public statement is true and she indeed intends to discover bat coronaviruses with a potential to cross-over to humans, how could she possibly overlook this extremely interesting finding of RaTG13?
If this RaTG13 was discovered SEVEN years ago in 2013, why did Shi not publish this astonishing finding earlier and yet let the 'less-attractive' viruses take the stage? Why did she decide to publish such a sequence only when the current outbreak took place and people started questioning the origin of the Wuhan coronavirus?
None of these makes sense. These facts only add to the suspicion — Zhengli Shi either was directly involved in the creation of this virus/bioweapon, or helped cover it up, or both. Of course, these facts also add to the claim that RaTG13 is a fake virus — it exists on Nature (the journal) but not in nature," the anonymous blogger writes.34
The blogger then goes on to dissect the genetic sequence RaTG13's spike protein, which "reveals clear evidence of human manipulation." (Again, Mosher offers a layman's overview35 of the data.) Martenson36 and Deigin's37 reviews of the viral genome also focus on the S2 spike protein, but they both focus on the spike protein found in SARS-CoV-2 (not the RaTG13 spike).
According to Martenson, the fact that SARS-CoV-2's spike protein has a furin cleavage site is "the smoking gun" that proves it was created in a lab. I invite you to review his easy-to-follow analysis in "The Smoking Gun Proving SARS-CoV-2 Is an Engineered Virus."
If the Nerd Has Power blogger is correct, and the bat virus RaTG13 was in fact fabricated in order to give the natural evolution theory of SARS-CoV-2 some credence, then the evidence for a man-made pandemic becomes all the more compelling. There's also other evidence that raise serious questions about the origin of this pandemic virus.
Other Evidence of Manipulation
In an earlier blog post, dated March 15, 2020, Nerd Has Power explains the importance of the S1 and S2 spikes of a given virus.38 In that post, the blogger also details significant changes found in the S1 portion of the SARS-CoV-2 spike protein, "which dictates which host a coronavirus targets," whereas much of the rest of the spike is very similar to the bat coronaviruses ZC45 and ZXC21. According to the blogger:39
"… the details of these differences and the way the human and the bat viruses differ from each other here in S1, in my and many other people's eyes, practically spell out the origin of the Wuhan coronavirus — it is created by people, not by nature."
In my opinion, the strongest pieces of evidence so far all point toward SARS-CoV-2 being a laboratory creation. How it got released, however, and why, remains to be determined.
The fact that the people responsible would want to cover it up is obvious, however, when you consider that the punishment in such an event could include life in prison for violating the Biological Weapons Anti-Terrorism Act of 1989.40
from Articles https://ift.tt/2XdxlfQ
via IFTTT
MKRdezign
Powered by Blogger.